This document discusses heart failure, including:
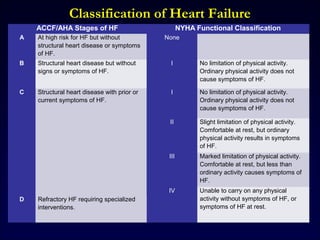
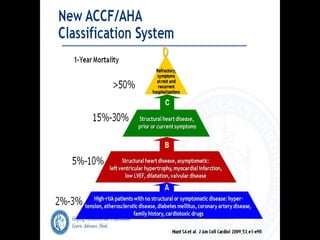
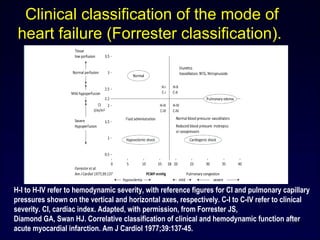
1. It provides classifications of heart failure stages and functional classifications according to ACCF/AHA and NYHA systems.
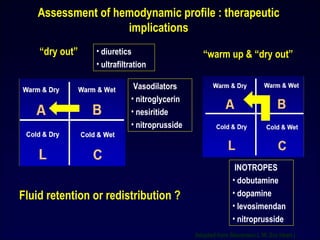
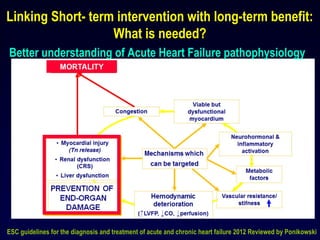
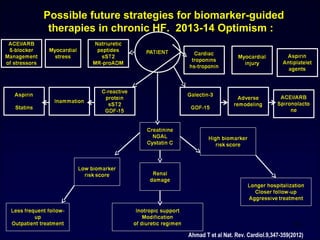
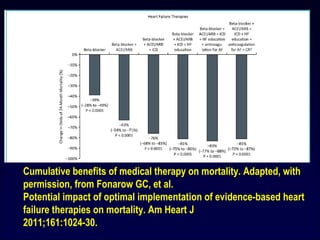
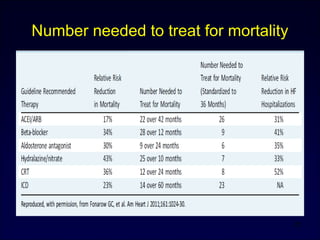
2. It outlines treatment approaches for different heart failure stages, including diuretics, vasodilators, inotropes, and approaches based on fluid retention status.
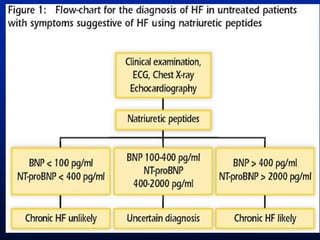
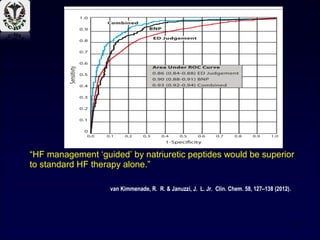
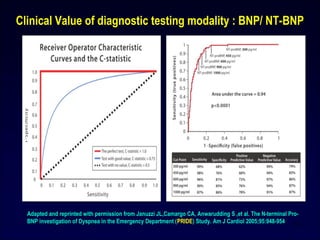
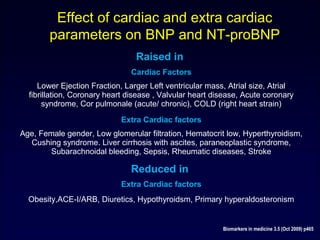
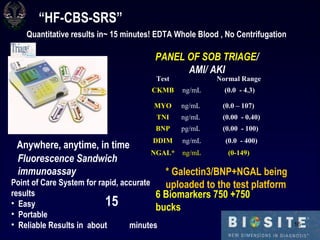
3. It discusses the use of biomarkers like BNP and NT-proBNP in diagnosing and managing heart failure and factors that can influence biomarker levels.





















![Heart failure – an update [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/heartfailureanupdateautosaved-110321012825-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)






















































































