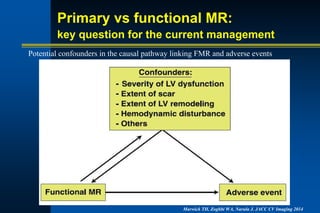
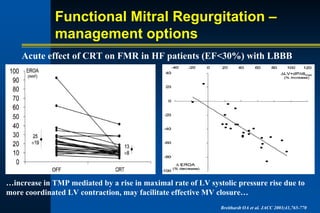
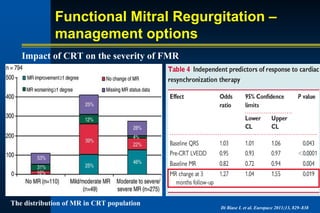
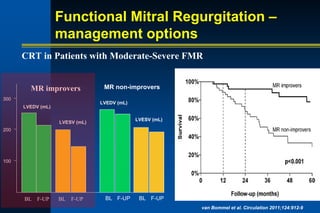
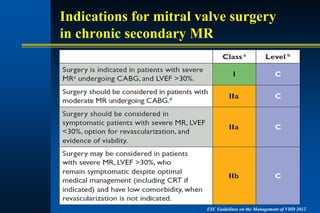
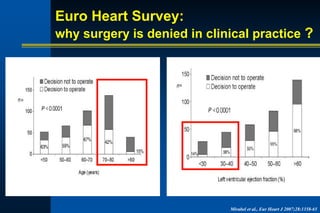
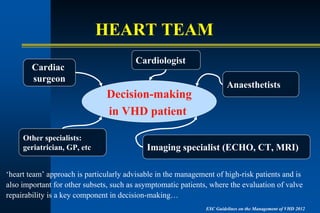
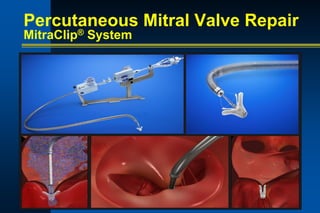
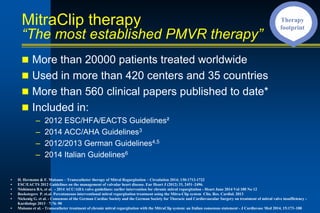
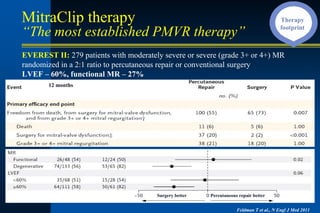
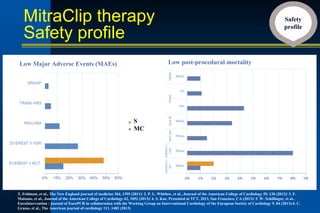
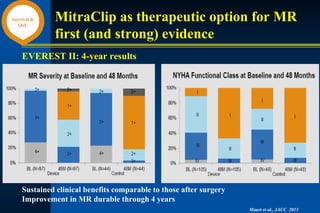
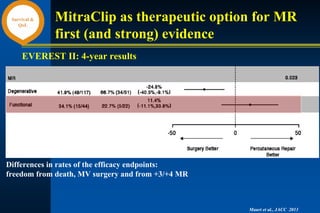
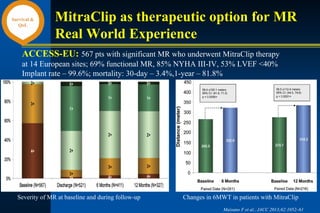
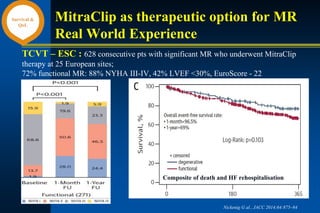
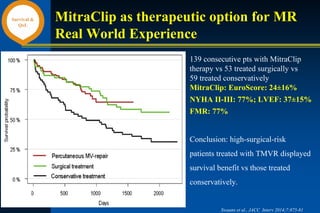
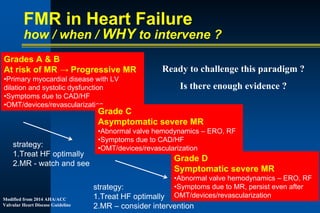
This document discusses the management of mitral regurgitation (MR) in heart failure patients. It explores the differences between primary and functional (secondary) MR, and notes that correcting primary MR may improve outcomes but the benefits are less clear for functional MR which is primarily a ventricular problem. The document reviews potential management options for MR in heart failure including optimal medical therapy, cardiac resynchronization therapy, surgery, and percutaneous techniques such as the MitraClip system. It presents evidence from studies on the acute effects of CRT and the impact of CRT on functional MR severity. It also discusses guidelines on indications for mitral valve surgery in chronic secondary MR and barriers to surgery.