Downloaded 104 times

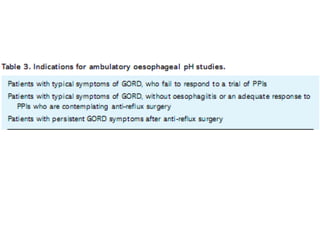
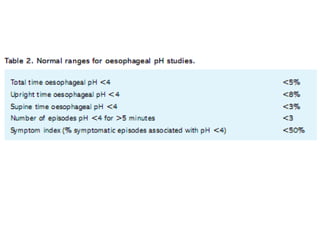
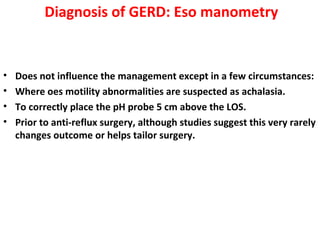

This document provides an overview of GERD (gastroesophageal reflux disease), including its prevalence, definitions, classifications, pathophysiology, clinical features, diagnosis and treatment. It notes that GERD is commonly underdiagnosed and discusses various testing and diagnostic methods. It also outlines approaches to treatment, including lifestyle changes, medications like PPIs and H2 blockers, and potentially surgery for severe cases that do not respond to medical management.







































































































