Downloaded 55 times



![Adding prokinetic medications to PPI?
One RCT comparing
Omeprazole 20 mg BID/day + domperidone 10 mg three times daily vs.omeprazole 20 mg twice daily found decreased symptoms with a meanimprovement using a validated symptom score.
However, a meta-analysis of 12 RCTs found that the combination of a prokineticand PPI did not improve symptoms and was associated with more adverseeffects than a PPI alone.
Katz PO, et al. Guidelines for the diagnosis and management of gastroesophageal reflux disease [published correction
appears in Am J Gastroenterol. 2013;108(10): 1672]. Am J Gastroenterol. 2013;108(3):308–328.](https://image.slidesharecdn.com/gerd-170906043911/85/Gerd-10-320.jpg)
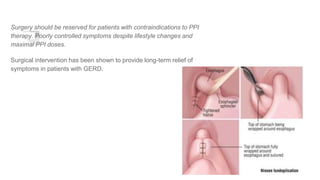
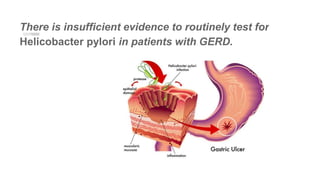

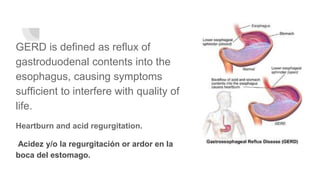
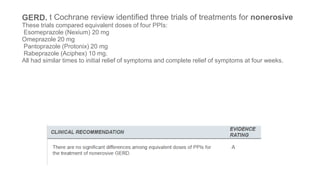
Gastroesophageal reflux disease (GERD) affects over 60 million Americans and is commonly diagnosed and treated by family physicians. GERD is defined as reflux of stomach contents into the esophagus, causing symptoms like heartburn and acid regurgitation. Proton pump inhibitors (PPIs) are highly effective at relieving GERD symptoms and different PPIs provide similar relief. Long-term PPI use may be associated with complications like hypomagnesemia, hip fractures, and pneumonia. Endoscopy is useful for diagnosing GERD complications but not sensitive for diagnosing GERD itself. Surgery should be reserved for severe cases that are poorly controlled by lifestyle changes and high doses



































































