Downloaded 138 times



![JensMartensson
18
Extracrevicular method Intracrevicular method ‘superficial’
[Loe & Holm-Pedersen]
Intracrevicular method
‘deep’ [Brill, 1958]](https://image.slidesharecdn.com/4gcf30919-191014184111/85/GINGIVAL-CREVICULAR-FLUID-18-320.jpg)
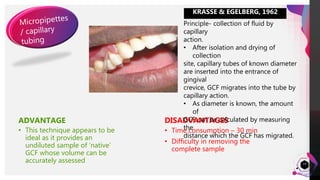
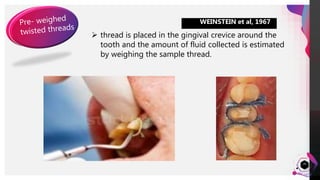
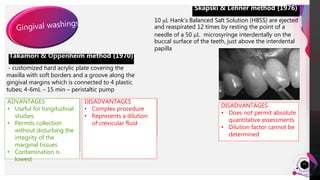
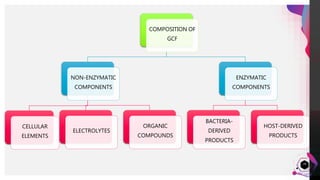
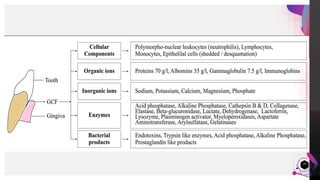
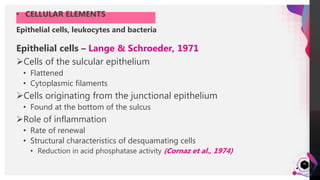
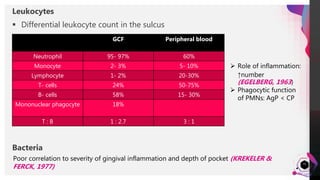


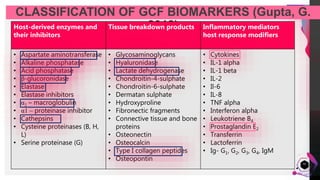


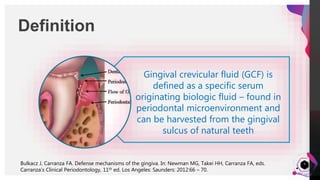
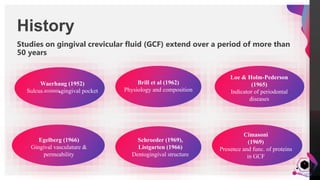
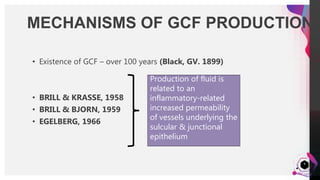
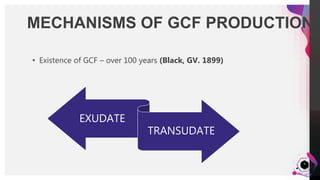
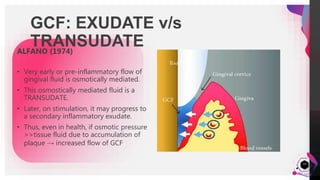
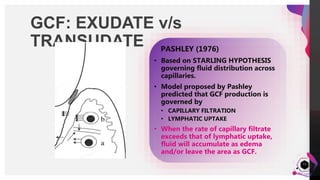
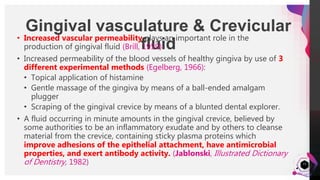
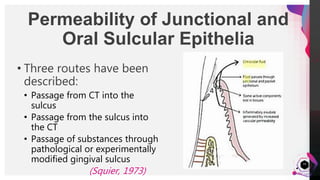
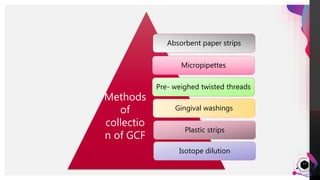
The document discusses gingival crevicular fluid (GCF), including its history of study over 50 years, mechanisms and factors affecting its production, methods of collection, composition, and clinical significance. GCF is a serum-like fluid found in the gingival sulcus that can be assessed to provide diagnostic information about periodontal health and disease. The document outlines the anatomy of the gingival crevice and epithelium, as well as various methods that have been used to collect and analyze GCF components.



















































































