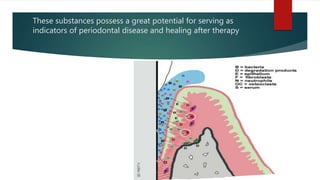
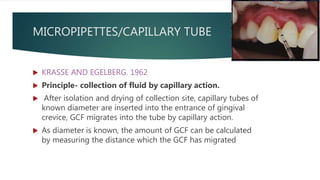
Gingival crevicular fluid (GCF) is a serum exudate found in the gingival sulcus. It forms due to an increase in capillary permeability and the osmotic gradient that causes interstitial fluid to accumulate in the sulcus. GCF contains substances from serum, leukocytes, periodontal tissues, and bacteria that can indicate periodontal disease status. It is collected using absorbent paper strips, threads, micropipettes, or lavage to analyze volume and composition. Elevated levels of enzymes, microbes, and metabolic products in GCF have been associated with periodontal tissue destruction.
























![PERIODONTAL WOUND HEALING [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/periodontalwoundhealingautosaved-240205115031-ce7a6d10-thumbnail.jpg?width=640&height=640&fit=bounds)


















































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
