![Case 2
A 75-year-old male presented with headache of six weeks' duration.
Pain was predominantly over the right hemicranium, with the
maximum being over the right temple. Pain was excruciating in
intensity. There was severe allodynia over the area. There was jaw
claudication. Constitutional symptoms were present. About two
weeks after the onset of headache, he developed blurred vision in
the right eye; an ophthalmological examination revealed anterior
ischemic optic neuropathy (AION). Examination and salient
laboratory findings are as tabulated in Table 1. Diagnosis of GCA was
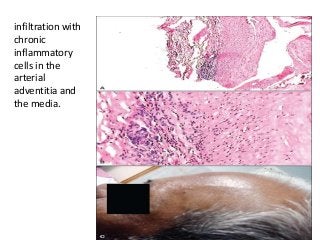
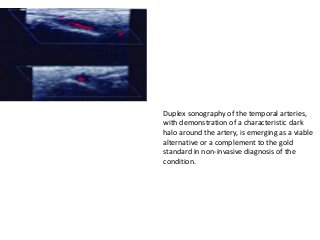
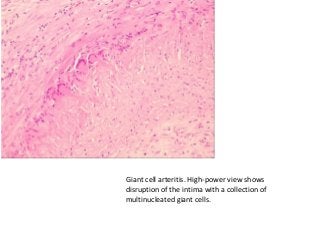
confirmed with STA biopsy [Figure 1]. He was treated with
intravenous methyl prednisolone, in a dose of 1 gm/day for three
days, followed by oral steroid in tapering doses. His headache and
constitutional symptoms improved rapidly. However, visual acuity
remained unchanged. He had recurrence of mild headache, three
months after he stopped the steroids by himself, and improved with
re- institution of steroid.](https://image.slidesharecdn.com/rheumatologygca-170216215748/85/Giant-cell-arteritis-polymyalgia-rheumatica-4-320.jpg?cb=1676625846)
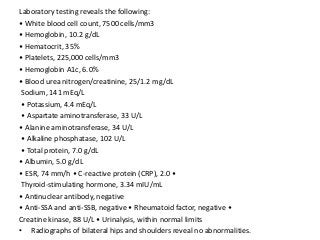
![Laboratory tests
1. mild anemia compatible with heterozygous
beta-thalassemia.
2. moderately high inflammation markers [ESR: 44
mm/h, CRP: 41.8 mg/L (normal values <5 mg/L)].
3. Kidney and liver function tests were within
normal range, and antinuclear and
antineutrophil cytoplasmic antibodies were
negative](https://image.slidesharecdn.com/rheumatologygca-170216215748/85/Giant-cell-arteritis-polymyalgia-rheumatica-12-320.jpg?cb=1676625846)

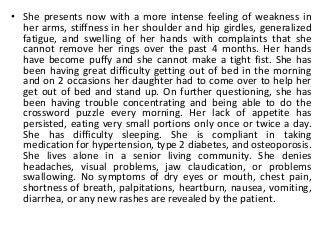
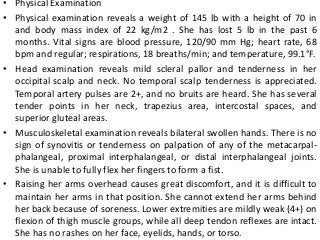
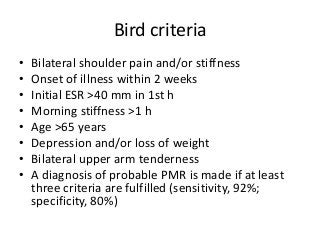
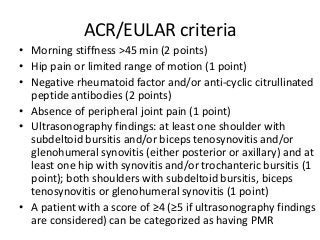
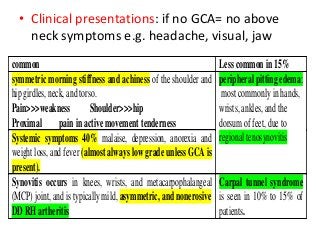
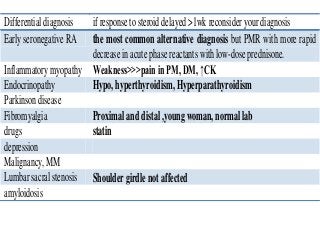

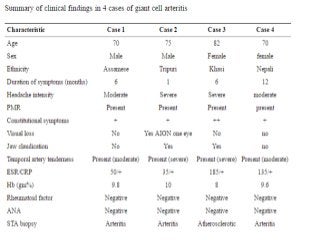
This document discusses giant cell arteritis (GCA) and polymyalgia rheumatica (PMR) through 5 case studies. It presents on a 70-year-old male initially diagnosed with PMR based on shoulder and back pain, who later developed headaches and temporal artery tenderness and was diagnosed with GCA. Another case outlines an elderly male with headaches, jaw claudication and vision loss diagnosed with GCA. Less common presentations of GCA involving neurological symptoms are also reviewed. The pathophysiology of GCA is described as an inflammatory process involving dendritic cells, T-lymphocytes and giant cells affecting temporal and other cranial arteries. Complications can include blindness, stroke and aortic aneurysms











































































































