This document discusses diabetes mellitus in pregnancy. It defines gestational diabetes as impaired glucose tolerance first recognized during the second or third trimester of pregnancy. Risk factors include family history of diabetes, obesity, and age over 30. During pregnancy, placental hormones increase insulin resistance and antagonize insulin effectiveness, raising blood sugar levels and potentially leading to hyperglycemia. Proper management includes monitoring blood sugar via fasting and post-meal tests, exercise, and treatment with insulin or oral medications if needed to control glucose levels and minimize risks to both mother and fetus.
This presentation is part of and education series to pediatric healthcare providers in Syria and it may be useful to all practitioners working in low resource settings.
Gestational diabetes Mellitus is defined as:
“Glucose intolerance of any severity with onset or first recognition during pregnancy”
This definition is applicable irrespective of whether the condition resolves after delivery or not.
It does not exclude the possibility that diabetes could have antedated pregnancy.
�
- gestational DM is critical metabolic disorder during pregnancy .
- According to a 2014 analysis by the Centers for Disease Control and Prevention, the prevalence of gestational diabetes is as high as 9.2%
- this presentation is about Gestational DM , introduction , diagnostic criteria , principles of approach and treatment and the sequels of such pregnancy and it`s effect of coming infant .
- this presentation is done by ; Dr. Nawras Mahir Farhan .
- References : most info.s in this presentation , from Dewhurst's Textbook of Obstetrics and Gynaecology, gynecology and obstetrics by ten teachers .
This presentation is part of and education series to pediatric healthcare providers in Syria and it may be useful to all practitioners working in low resource settings.
Gestational diabetes Mellitus is defined as:
“Glucose intolerance of any severity with onset or first recognition during pregnancy”
This definition is applicable irrespective of whether the condition resolves after delivery or not.
It does not exclude the possibility that diabetes could have antedated pregnancy.
�
- gestational DM is critical metabolic disorder during pregnancy .
- According to a 2014 analysis by the Centers for Disease Control and Prevention, the prevalence of gestational diabetes is as high as 9.2%
- this presentation is about Gestational DM , introduction , diagnostic criteria , principles of approach and treatment and the sequels of such pregnancy and it`s effect of coming infant .
- this presentation is done by ; Dr. Nawras Mahir Farhan .
- References : most info.s in this presentation , from Dewhurst's Textbook of Obstetrics and Gynaecology, gynecology and obstetrics by ten teachers .
The Primary Care Physician's guide to management of Pregnancy DiabetesHanifullah Khan
A guide on the screening, diagnosis and management of diabetes in pregnancy aimed at facilitating the handling of this condition in a primary care setting. Includes details on medications and dosages
A comprehensive guide to the management of hyperglycaemia in pregnancy aimed at the primary care physician and based on latest evidenced based criteria. Includes information from latest studies such as HAPO study and ACHOIS, and involves guidelines from the IADPSG, ADA, WHO and Malaysia.
Pulmonary Thromboembolism - etilogy, types, medical- Surgical and nursing man...VarunMahajani
Disruption of blood supply to lung alveoli due to blockage of one or more pulmonary blood vessels is called as Pulmonary thromboembolism. In this presentation we will discuss its causes, types and its management in depth.
Couples presenting to the infertility clinic- Do they really have infertility...Sujoy Dasgupta
Dr Sujoy Dasgupta presented the study on "Couples presenting to the infertility clinic- Do they really have infertility? – The unexplored stories of non-consummation" in the 13th Congress of the Asia Pacific Initiative on Reproduction (ASPIRE 2024) at Manila on 24 May, 2024.
Explore natural remedies for syphilis treatment in Singapore. Discover alternative therapies, herbal remedies, and lifestyle changes that may complement conventional treatments. Learn about holistic approaches to managing syphilis symptoms and supporting overall health.
Tom Selleck Health: A Comprehensive Look at the Iconic Actor’s Wellness Journeygreendigital
Tom Selleck, an enduring figure in Hollywood. has captivated audiences for decades with his rugged charm, iconic moustache. and memorable roles in television and film. From his breakout role as Thomas Magnum in Magnum P.I. to his current portrayal of Frank Reagan in Blue Bloods. Selleck's career has spanned over 50 years. But beyond his professional achievements. fans have often been curious about Tom Selleck Health. especially as he has aged in the public eye.
Follow us on: Pinterest
Introduction
Many have been interested in Tom Selleck health. not only because of his enduring presence on screen but also because of the challenges. and lifestyle choices he has faced and made over the years. This article delves into the various aspects of Tom Selleck health. exploring his fitness regimen, diet, mental health. and the challenges he has encountered as he ages. We'll look at how he maintains his well-being. the health issues he has faced, and his approach to ageing .
Early Life and Career
Childhood and Athletic Beginnings
Tom Selleck was born on January 29, 1945, in Detroit, Michigan, and grew up in Sherman Oaks, California. From an early age, he was involved in sports, particularly basketball. which played a significant role in his physical development. His athletic pursuits continued into college. where he attended the University of Southern California (USC) on a basketball scholarship. This early involvement in sports laid a strong foundation for his physical health and disciplined lifestyle.
Transition to Acting
Selleck's transition from an athlete to an actor came with its physical demands. His first significant role in "Magnum P.I." required him to perform various stunts and maintain a fit appearance. This role, which he played from 1980 to 1988. necessitated a rigorous fitness routine to meet the show's demands. setting the stage for his long-term commitment to health and wellness.
Fitness Regimen
Workout Routine
Tom Selleck health and fitness regimen has evolved. adapting to his changing roles and age. During his "Magnum, P.I." days. Selleck's workouts were intense and focused on building and maintaining muscle mass. His routine included weightlifting, cardiovascular exercises. and specific training for the stunts he performed on the show.
Selleck adjusted his fitness routine as he aged to suit his body's needs. Today, his workouts focus on maintaining flexibility, strength, and cardiovascular health. He incorporates low-impact exercises such as swimming, walking, and light weightlifting. This balanced approach helps him stay fit without putting undue strain on his joints and muscles.
Importance of Flexibility and Mobility
In recent years, Selleck has emphasized the importance of flexibility and mobility in his fitness regimen. Understanding the natural decline in muscle mass and joint flexibility with age. he includes stretching and yoga in his routine. These practices help prevent injuries, improve posture, and maintain mobilit
263778731218 Abortion Clinic /Pills In Harare ,sisternakatoto
263778731218 Abortion Clinic /Pills In Harare ,ABORTION WOMEN’S CLINIC +27730423979 IN women clinic we believe that every woman should be able to make choices in her pregnancy. Our job is to provide compassionate care, safety,affordable and confidential services. That’s why we have won the trust from all generations of women all over the world. we use non surgical method(Abortion pills) to terminate…Dr.LISA +27730423979women Clinic is committed to providing the highest quality of obstetrical and gynecological care to women of all ages. Our dedicated staff aim to treat each patient and her health concerns with compassion and respect.Our dedicated group ABORTION WOMEN’S CLINIC +27730423979 IN women clinic we believe that every woman should be able to make choices in her pregnancy. Our job is to provide compassionate care, safety,affordable and confidential services. That’s why we have won the trust from all generations of women all over the world. we use non surgical method(Abortion pills) to terminate…Dr.LISA +27730423979women Clinic is committed to providing the highest quality of obstetrical and gynecological care to women of all ages. Our dedicated staff aim to treat each patient and her health concerns with compassion and respect.Our dedicated group of receptionists, nurses, and physicians have worked together as a teamof receptionists, nurses, and physicians have worked together as a team wwww.lisywomensclinic.co.za/
HOT NEW PRODUCT! BIG SALES FAST SHIPPING NOW FROM CHINA!! EU KU DB BK substit...GL Anaacs
Contact us if you are interested:
Email / Skype : kefaya1771@gmail.com
Threema: PXHY5PDH
New BATCH Ku !!! MUCH IN DEMAND FAST SALE EVERY BATCH HAPPY GOOD EFFECT BIG BATCH !
Contact me on Threema or skype to start big business!!
Hot-sale products:
NEW HOT EUTYLONE WHITE CRYSTAL!!
5cl-adba precursor (semi finished )
5cl-adba raw materials
ADBB precursor (semi finished )
ADBB raw materials
APVP powder
5fadb/4f-adb
Jwh018 / Jwh210
Eutylone crystal
Protonitazene (hydrochloride) CAS: 119276-01-6
Flubrotizolam CAS: 57801-95-3
Metonitazene CAS: 14680-51-4
Payment terms: Western Union,MoneyGram,Bitcoin or USDT.
Deliver Time: Usually 7-15days
Shipping method: FedEx, TNT, DHL,UPS etc.Our deliveries are 100% safe, fast, reliable and discreet.
Samples will be sent for your evaluation!If you are interested in, please contact me, let's talk details.
We specializes in exporting high quality Research chemical, medical intermediate, Pharmaceutical chemicals and so on. Products are exported to USA, Canada, France, Korea, Japan,Russia, Southeast Asia and other countries.
NVBDCP.pptx Nation vector borne disease control programSapna Thakur
NVBDCP was launched in 2003-2004 . Vector-Borne Disease: Disease that results from an infection transmitted to humans and other animals by blood-feeding arthropods, such as mosquitoes, ticks, and fleas. Examples of vector-borne diseases include Dengue fever, West Nile Virus, Lyme disease, and malaria.
Ozempic: Preoperative Management of Patients on GLP-1 Receptor Agonists Saeid Safari
Preoperative Management of Patients on GLP-1 Receptor Agonists like Ozempic and Semiglutide
ASA GUIDELINE
NYSORA Guideline
2 Case Reports of Gastric Ultrasound
Title: Sense of Smell
Presenter: Dr. Faiza, Assistant Professor of Physiology
Qualifications:
MBBS (Best Graduate, AIMC Lahore)
FCPS Physiology
ICMT, CHPE, DHPE (STMU)
MPH (GC University, Faisalabad)
MBA (Virtual University of Pakistan)
Learning Objectives:
Describe the primary categories of smells and the concept of odor blindness.
Explain the structure and location of the olfactory membrane and mucosa, including the types and roles of cells involved in olfaction.
Describe the pathway and mechanisms of olfactory signal transmission from the olfactory receptors to the brain.
Illustrate the biochemical cascade triggered by odorant binding to olfactory receptors, including the role of G-proteins and second messengers in generating an action potential.
Identify different types of olfactory disorders such as anosmia, hyposmia, hyperosmia, and dysosmia, including their potential causes.
Key Topics:
Olfactory Genes:
3% of the human genome accounts for olfactory genes.
400 genes for odorant receptors.
Olfactory Membrane:
Located in the superior part of the nasal cavity.
Medially: Folds downward along the superior septum.
Laterally: Folds over the superior turbinate and upper surface of the middle turbinate.
Total surface area: 5-10 square centimeters.
Olfactory Mucosa:
Olfactory Cells: Bipolar nerve cells derived from the CNS (100 million), with 4-25 olfactory cilia per cell.
Sustentacular Cells: Produce mucus and maintain ionic and molecular environment.
Basal Cells: Replace worn-out olfactory cells with an average lifespan of 1-2 months.
Bowman’s Gland: Secretes mucus.
Stimulation of Olfactory Cells:
Odorant dissolves in mucus and attaches to receptors on olfactory cilia.
Involves a cascade effect through G-proteins and second messengers, leading to depolarization and action potential generation in the olfactory nerve.
Quality of a Good Odorant:
Small (3-20 Carbon atoms), volatile, water-soluble, and lipid-soluble.
Facilitated by odorant-binding proteins in mucus.
Membrane Potential and Action Potential:
Resting membrane potential: -55mV.
Action potential frequency in the olfactory nerve increases with odorant strength.
Adaptation Towards the Sense of Smell:
Rapid adaptation within the first second, with further slow adaptation.
Psychological adaptation greater than receptor adaptation, involving feedback inhibition from the central nervous system.
Primary Sensations of Smell:
Camphoraceous, Musky, Floral, Pepperminty, Ethereal, Pungent, Putrid.
Odor Detection Threshold:
Examples: Hydrogen sulfide (0.0005 ppm), Methyl-mercaptan (0.002 ppm).
Some toxic substances are odorless at lethal concentrations.
Characteristics of Smell:
Odor blindness for single substances due to lack of appropriate receptor protein.
Behavioral and emotional influences of smell.
Transmission of Olfactory Signals:
From olfactory cells to glomeruli in the olfactory bulb, involving lateral inhibition.
Primitive, less old, and new olfactory systems with different path
3. INTRODUCTION
Diabetes Mellitus is a endocrine and
metabolic disorder in which inability in
carbohydrate ,fat and protien resulting
in raised blood glucose level .
4. Diabetes Mellitus In
Pregnancy
• Diabetes Mellitus is a common medical
disorder encounter in pregnancy.
• Pregnancy is a diabetogenic state due to
insulin resistance increase during
pregnancy .
• Placental hormones are increase during
pregnancy to disturbed insulin action.
5. INCEDENCE
.
•Diabetes remains the 7th leading cause of
death in the united states in 2010.
• According to the National Center for
Heath Statistics [2004] ,iabetes now occurs
in approximately 4 – 14 percent women.
•10 to 20 precent of patient with diabetes
are geststional diabetes.
6. TYPES
Diabetes mellites in pregnancy are 2
types =
1. Pre-gestational Diabetes Mellietes
1. Gestational Diabetes Mellietes
7. 1. Pre-Gestational Diabetes
Mellitus
• In which the diabetes
daigenosed before pregnancy.
• There are mainly 2 types.
1. Type -1 diabetes mellitus
2. Type -2 diabetes mellitus
8. Type-1 Diabetes Mellitus
Also known as the-
•Insulin Dependent Diabetes Mellitus
[IDDM].
•Juvenile Diabetes Mellitus
•It characterized by loss of the insulin
–producing beta cells of the pancreas
leading to insulin deficiency .
9. Pathophysiology and
Risk factors
.
Risk factors =
•Genetic
•Environmental
•Viral infection
Pathophysiology=
•Autoimmune reaction in which the beta
cells that produce insulinare destroyed.
•Alpha cells produce excess glucons
11. Type-2 Diabetes Mellitus
•Also known as Non Insulin Diabetes Mellitus[
NIDDM].
• Type 2 is charactrised by the presens of insulin are
low ,high ,normal and beta cell disfunctioning.
•Type 2 are most common type of diabetes 95 cases.
Risk factors=
•Obesity
•Physical activity
•Family history
•Intacke of high calorie diet
15. DEFINITION
• The word gastation actually refers to
during pregnancy
• Gastational diabetes mellitus is the most
common medical complicatin of
pregnancy
• GDM define as a impaired glucose
tolerence with 1st recognised druring 2&3
trimester(24to28week) of pregnancy
16. RISK FACTORS
Previous history of GDM
positive family history of DM type2
High risk group(aferican
americans,asian american)
Over age > 30 years
Smoking
Obesity
17.
18. HORMONAL CHANGES
PLACENTA
The placenta act as a endocrine organ producing
several important hormones during pregnancy
Placenta produce variety of hormonrs
Steroid
Protien
DURING THE FIRST TRIMESTER
Carpos luteum placenta secreat esteroid hormone
Esteron
progestron
19. •Estrogan and prosteron level are raise in blood
•These hormones estiulates the beta-cell hyperplacia
to secreat insulin
•Promote increase glycogan store
•Decrease hepatic production of glucose
•lead to decrease fasting blood gluse level in the 1st
trimester
20. DURING 2&3 TRIMESTER
*Placenta secreat daibetogenic and protin hormone
Human placental lectose
Estrogen and progestron
Placental insulinase
Increase hepatic glucose production
Decrease hepatic glycogan store
These hormone antagonise insuline effectiveness
Raising placenta hormone increase insulin
registance
Leading to hyperglycemia occuse after meals.
21.
22. PATHOPHYSIOLOGY
• Due to etiological factoes
• During 2&3 trimaster screat placental hormone
(Human placental lectose ,Estrogen and progestron
,Placental insulinase)
these hormone antagonised effect for insulin
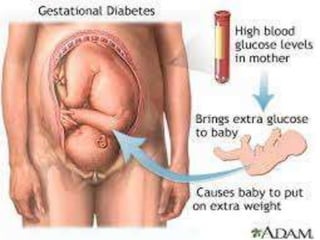
increase blood suger level
Body dose not made insulin properly
Matenal blood glucose in fetas throgh placenta
Fetal hyperglycemia
Activated pancreatic hyperplasia of beta-
cell(12week start insulin production)
Insulin increase in fetus
23. EFFECT OF DAIBETES ON PRTEGNANC
• MATENAL EFFECT
• IN PREGNANCY
• Abortion
• Infection
• Prterm labor
• Hypertansion
• Plyhdraminos
• DURING LABOUR
• Sholder distocia
• Prineal injuries
29. INVESTIGATION
• URINE CULTURE
• Should be done at the initial visit at 4-6week
interval to rule out asymptomatic bactoriuria.
• OPTHALMOLOGICAL EXAMINATION
• this is performed in all daibetics at the intial
antenatal examination and develop retinal changes
• RENAL FACTION
• A base line serum cretinine is optain at in the initial
visit and value is more than 0.8 mg/dl .
• Renal fuction is assesd every 4week
• ECG : suspected ischemic heart disease patient
30. MATERNAL SERUM ALFA FECTOPROTIEN:
Estimation is done between 16&20 weeks to screen
the nural tube defect
ULTRASOUND :it is indicate in the 1st trimester for
acurate dating of pregnancy
In eary growth lag ina pregatationa daibetes is an
indicate of a fetal malformation and early abortion
2nd trimester : detail anomalies sacle is perform abt
18-20 weeks
Fetal ecocardiography to rule out cardic anomalies is
done aroud 20-24weeks.
3red trimester: monitor macrosomia .
33. (2)EXERCISE
•Exercise is an important component in maitaining
glucose control
•Improves physical and psycological weelbeing of the
patient
Exercise must be avoided at the peak time of insulin
action.
Exercise sach as
Deepbrithing
Walking
yoga
34. (3)PHARMACOLOGICAL
INSULIN INFUTION:
If a contineously inslin infution is needed,25units of
regular insulin are added to 25mg of normal saline
The IV rate and supplimantal regular insuline based
on every 1to2 hr capillary boold glucose value
INTERMITENT SUBCUTINEOUS INSULIN