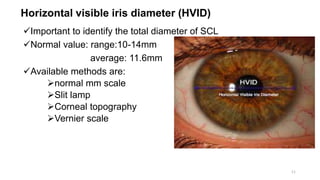
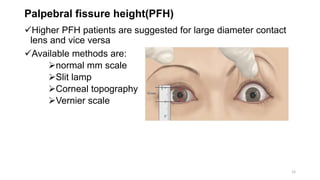
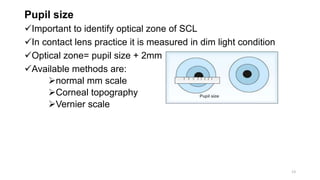
This presentation discusses the process of fitting soft contact lenses. It begins with defining soft contact lenses and outlining the objectives of understanding fitting steps and assessment. Baseline measurements are taken, including HVID, keratometry, and refraction. Trial lenses are selected based on these measurements. Fitting is then assessed based on criteria like movement, centration, and comfort response. Ideal fits show full corneal coverage and clear vision. Modifications may be made by altering the base curve, diameter, or thickness if needed. The proper fitting of contact lenses is important to ensure comfort and good vision.
























![Optics of contact lens and nomenclature copy [repaired] (1)](https://cdn.slidesharecdn.com/ss_thumbnails/opticsofcontactlensandnomenclature-copyrepaired1-170218054900-thumbnail.jpg?width=640&height=640&fit=bounds)













































