
Download to read offline

![Glasgow Coma Scale
The Glasgow Coma Scale (GCS) is
used to describe the general level of consciousness in
patients with traumatic brain injury (TBI) and to
define broad categories of head injury. [1] The GCS is
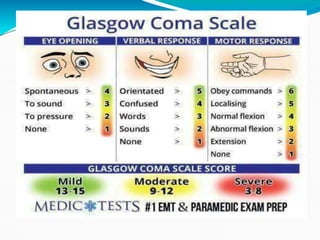
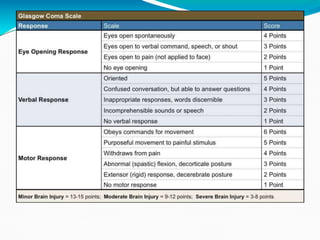
divided into 3 categories, eye opening (E), motor
response (M), and verbal response (V). The score is
determined by the sum of the score in each of the 3
categories, with a maximum score of 15 and a minimum
score of 3.](https://image.slidesharecdn.com/gcs-scte-221124054819-4bb45062/85/GCS-SCTE-ppt-2-320.jpg)
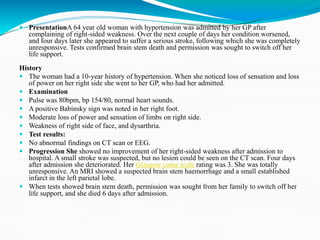
The Glasgow Coma Scale (GCS) evaluates consciousness levels in patients with traumatic brain injury, comprising three categories: eye opening, motor response, and verbal response, with a scoring range of 3 to 15. A clinical case is presented involving a 64-year-old woman with hypertension who experienced a stroke, leading to brain stem death and subsequent discontinuation of life support. The document includes detailed scoring criteria for GCS and describes the patient's symptoms, examination findings, and test results.























































































