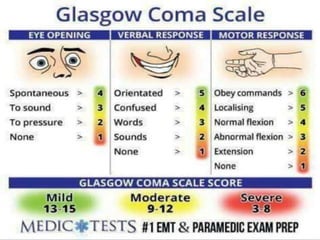
The Glasgow Coma Scale (GCS) is a neurological scale used to assess consciousness after brain injury. It evaluates eye opening, verbal response, and motor response on a scale of 3 to 15, with lower scores indicating worse condition. The GCS was developed in 1974 and provides a standardized way to record a patient's state and classify brain injuries as mild, moderate or severe based on the total score. Limitations include inability to fully assess intubated or facially injured patients.









































![glasgow coma scale gcs 2 [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/gcs2autosaved-260117045741-a747a447-thumbnail.jpg?width=640&height=640&fit=bounds)


























