Downloaded 15 times


































The Glasgow Coma Scale (GCS) is a neurological scale used to assess level of consciousness. It evaluates eye opening, verbal response, and motor response on a scale of 3-15. Though widely used, it has limitations like not assessing brainstem function or distinguishing mild injuries. Several other scales have been developed, like the FOUR score which also evaluates brainstem reflexes and eye movements, and the Glasgow Outcome Scale which measures long-term recovery. The GCS remains valuable for initial assessment, monitoring changes, and predicting outcomes in various conditions like traumatic brain injury and stroke.
Overview of neurological scales including GCS, its historical introduction, and significance.
Detailed explanation of GCS components: eye opening, verbal response, and motor response evaluations.
GCS application in children, outcomes for head trauma and intracranial hemorrhage, and age-specific considerations.
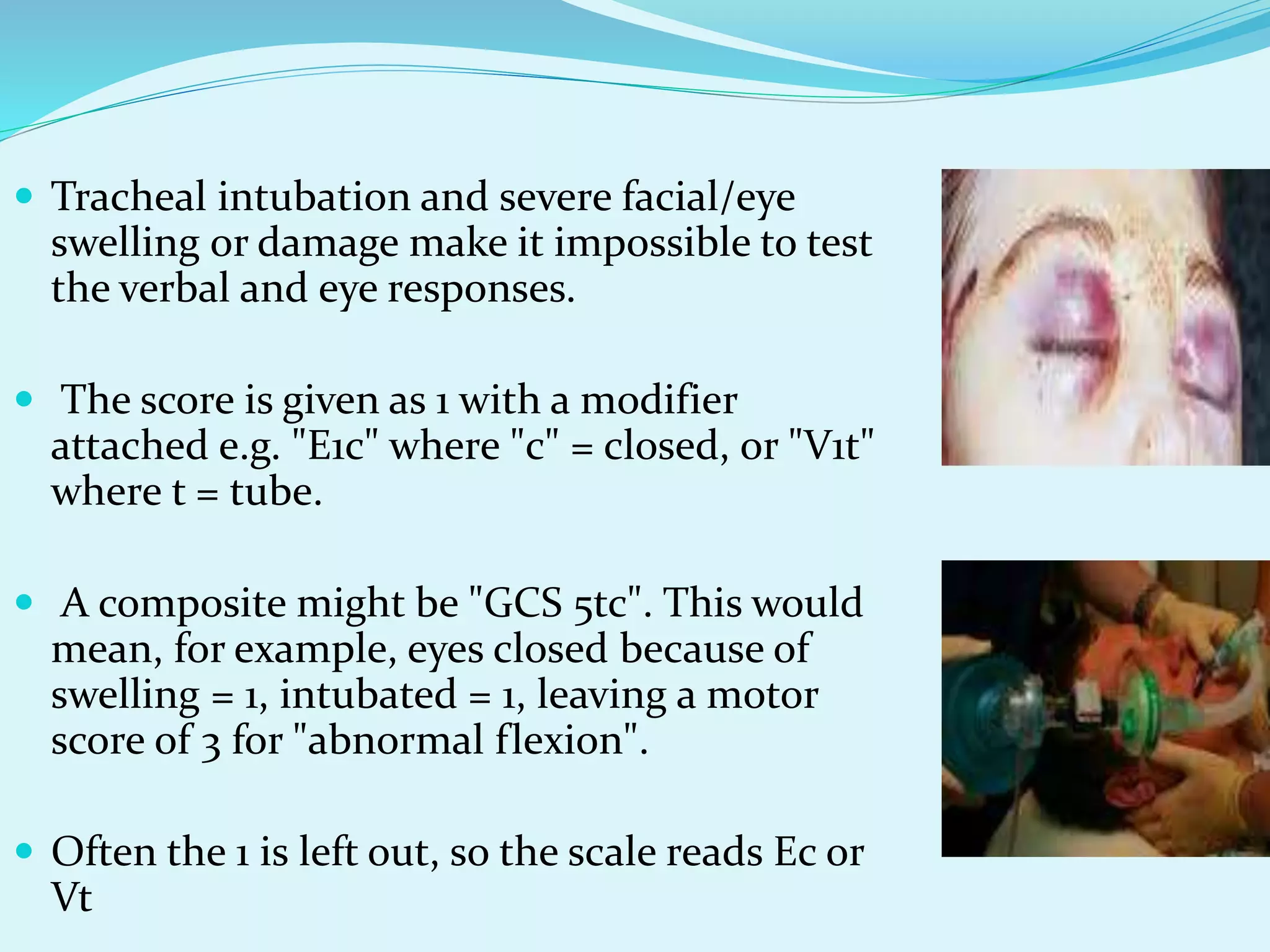
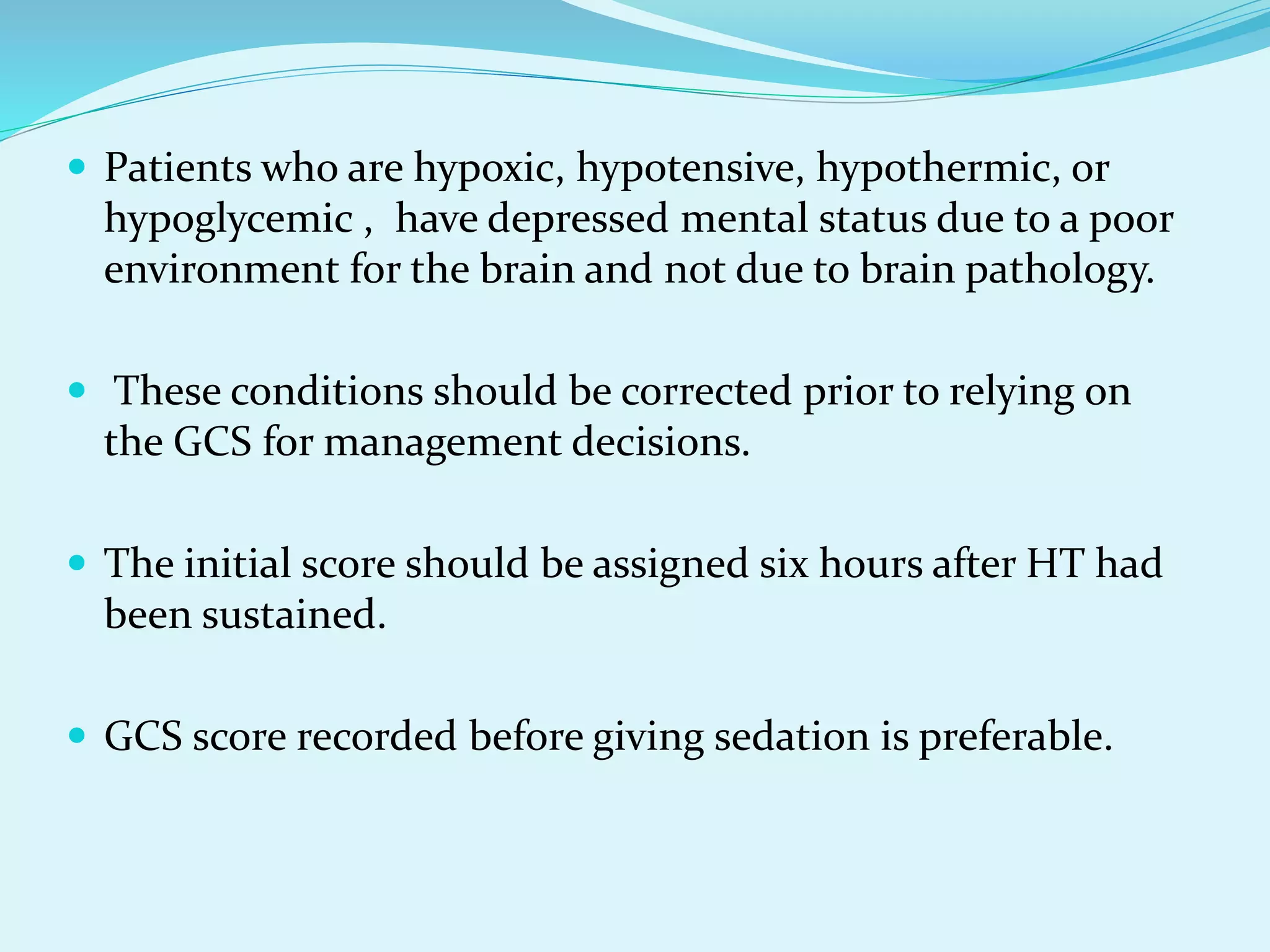
Factors affecting GCS scores, including sedation, injuries, and environmental conditions impacting assessment.
Key applications of GCS in monitoring coma, triage, detecting complications, and influencing clinical decisions.
GCS's role in assessing head trauma severity, imaging recommendations, and outcomes in stroke cases.
Limitations of GCS in measuring concussion severity, introduction of GCS-Extended for better assessment.
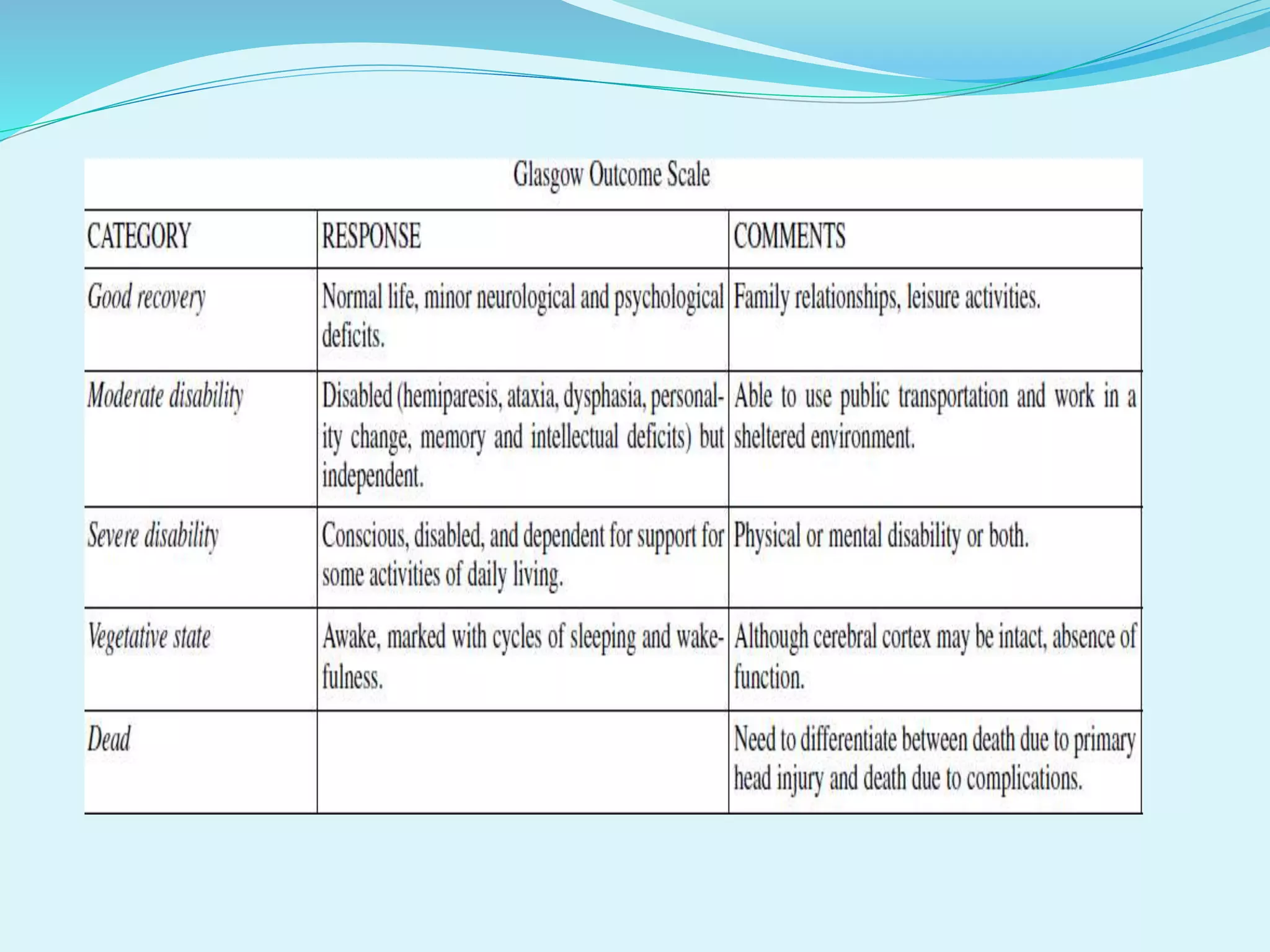
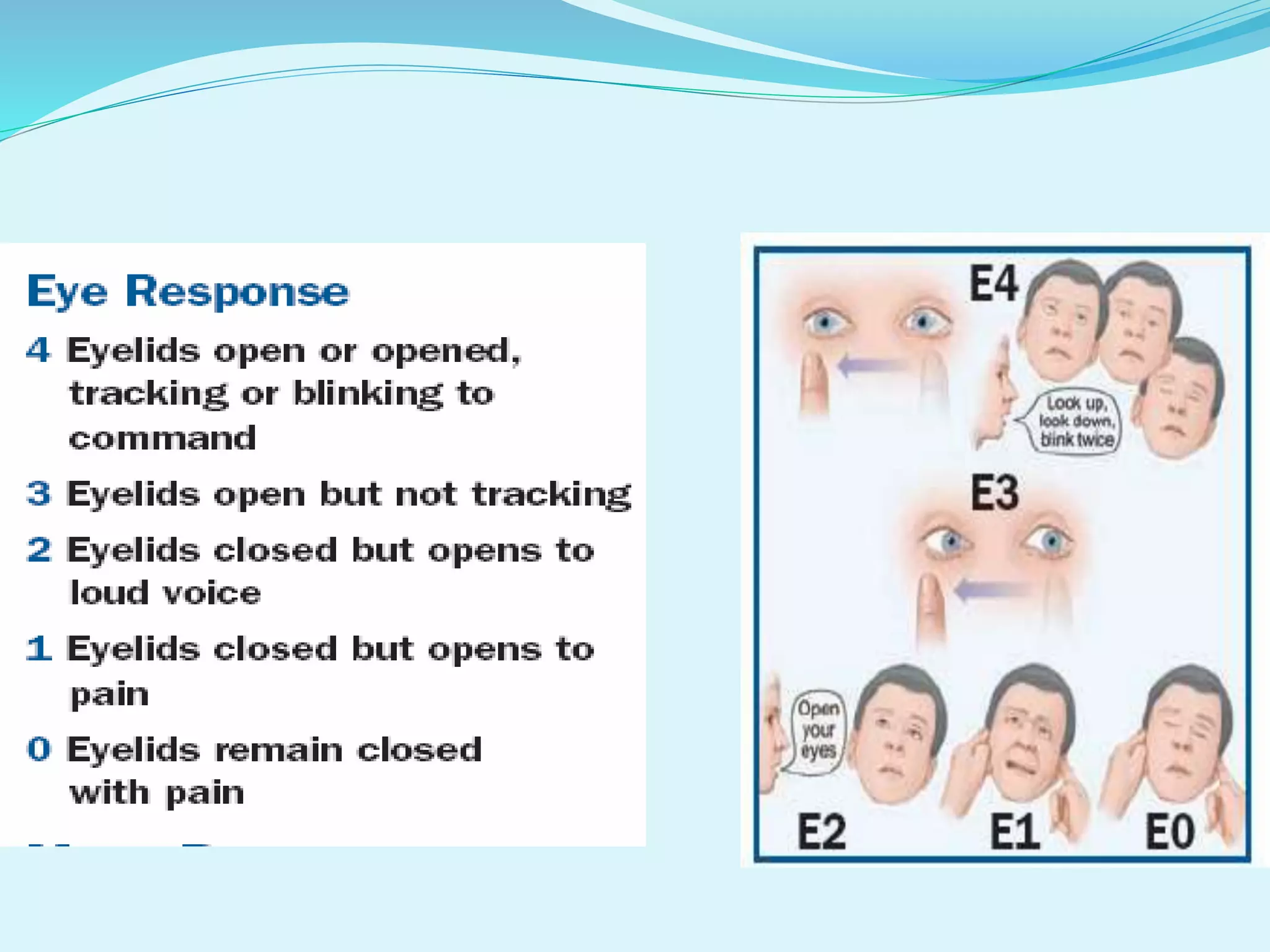
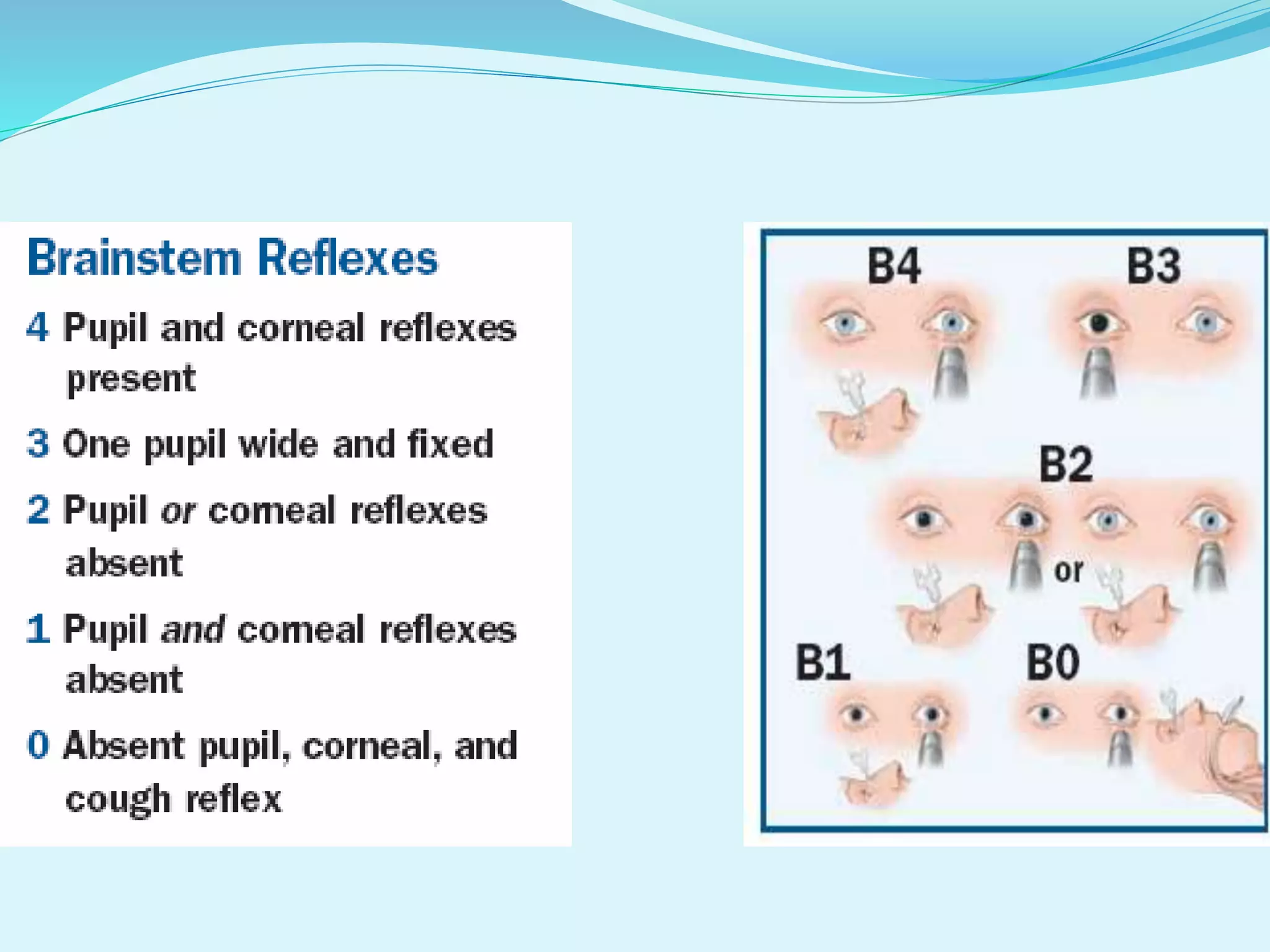
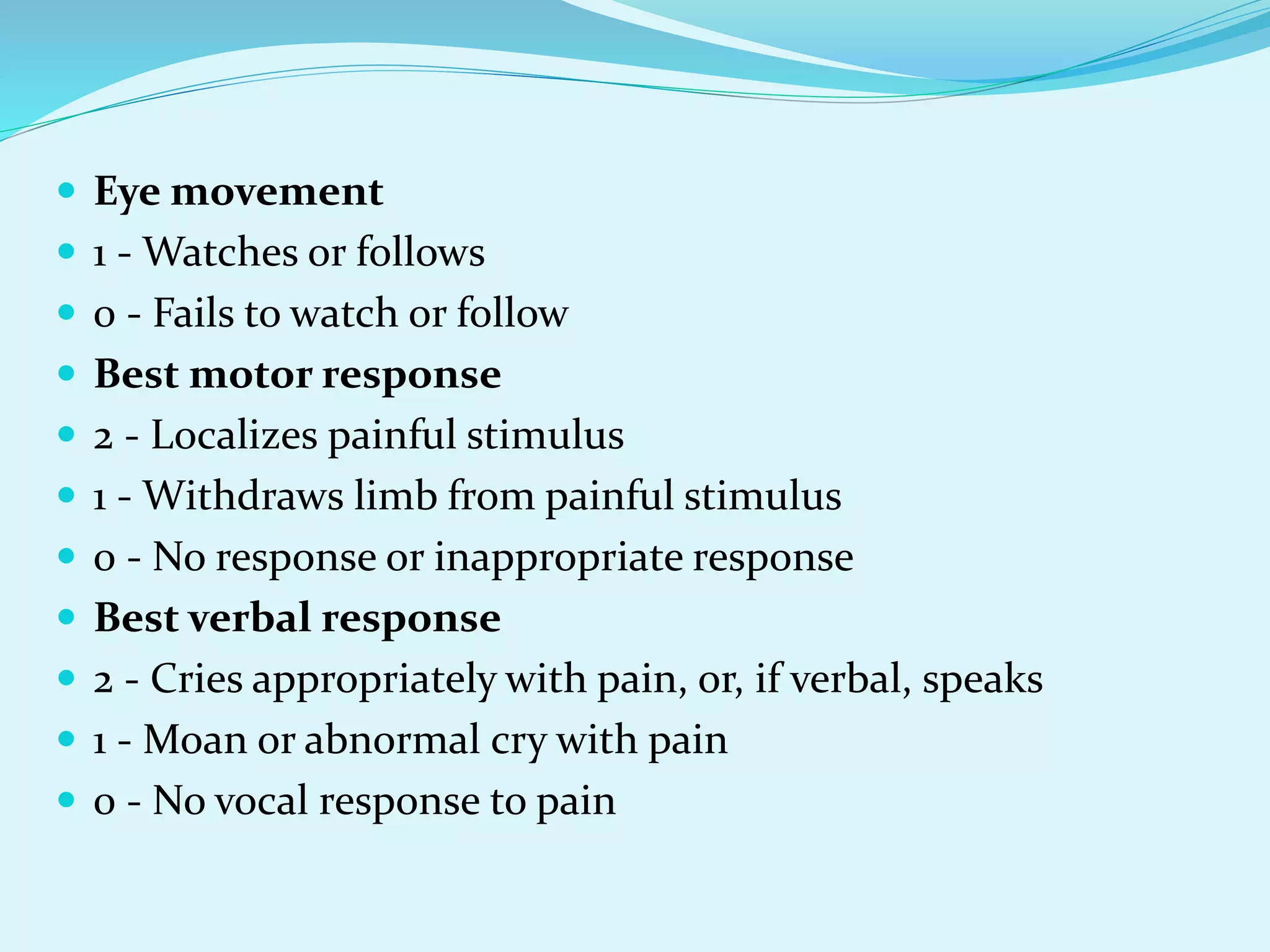
Discussion on Glasgow Outcome Score, FOUR Score, WFNS, Blantyre, and Rancho Los Amigos Scale for coma assessment.
GCS's role in assessing neurological status and the need for thorough examination alongside proper scoring.























































































