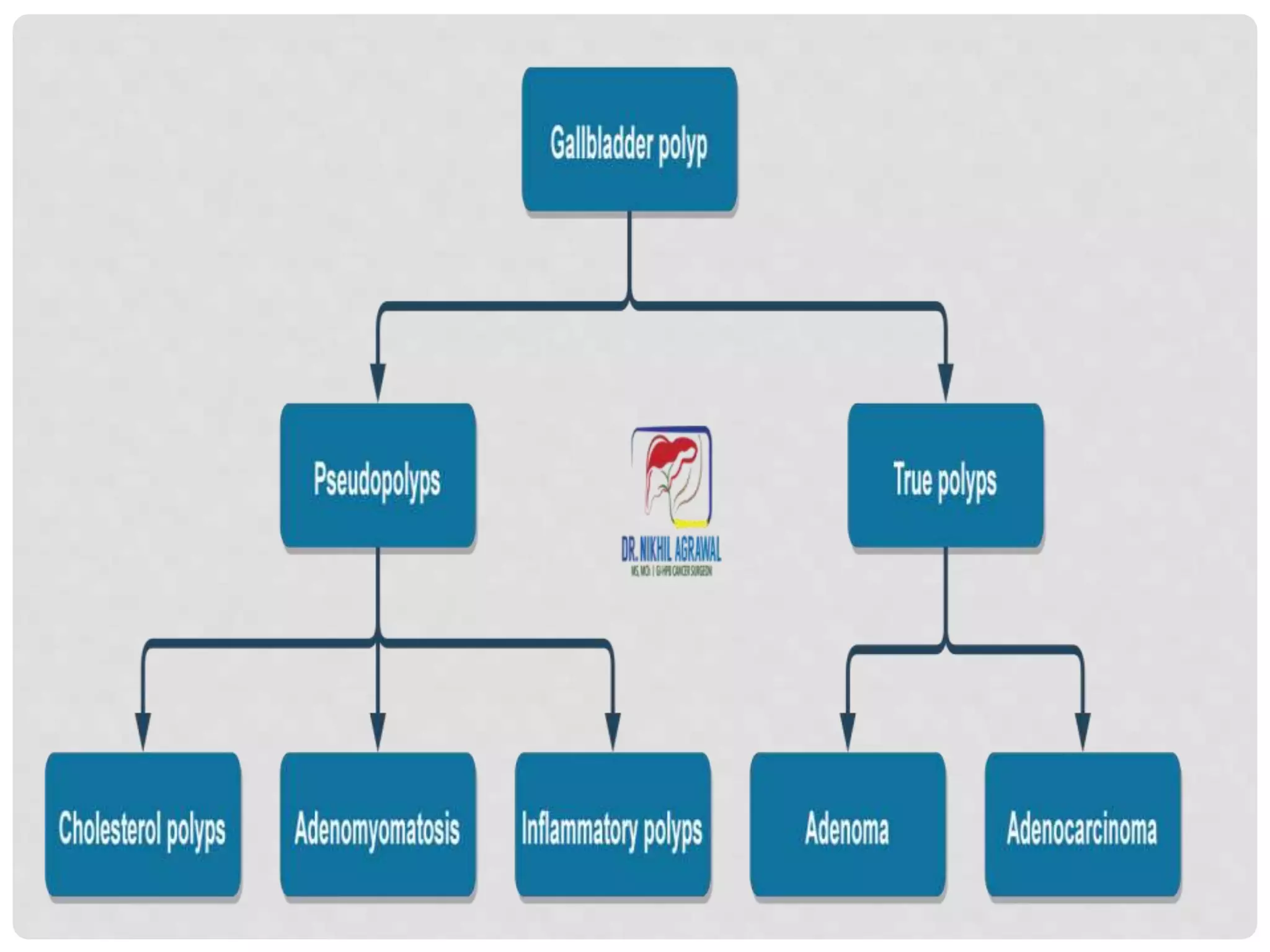
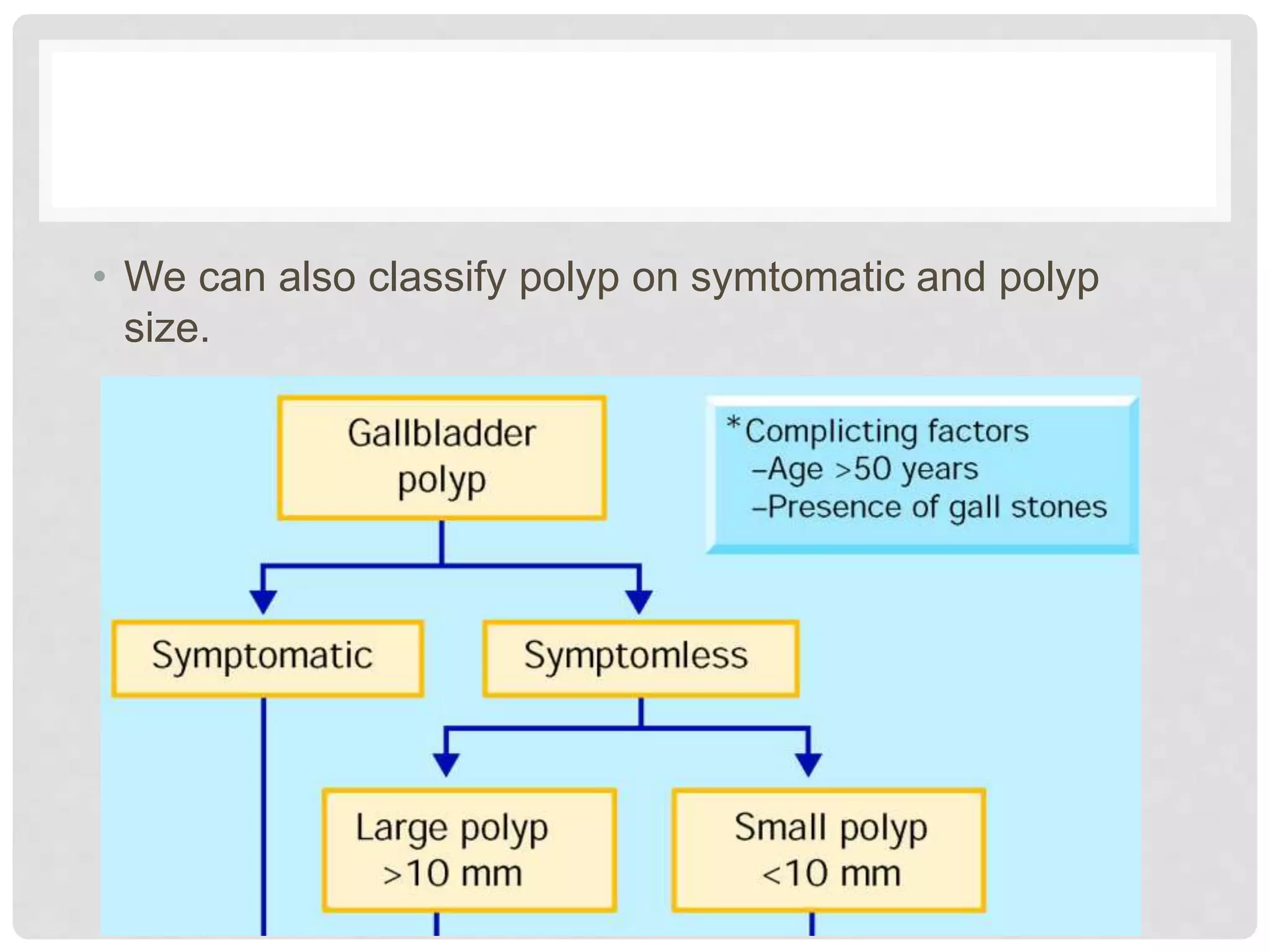
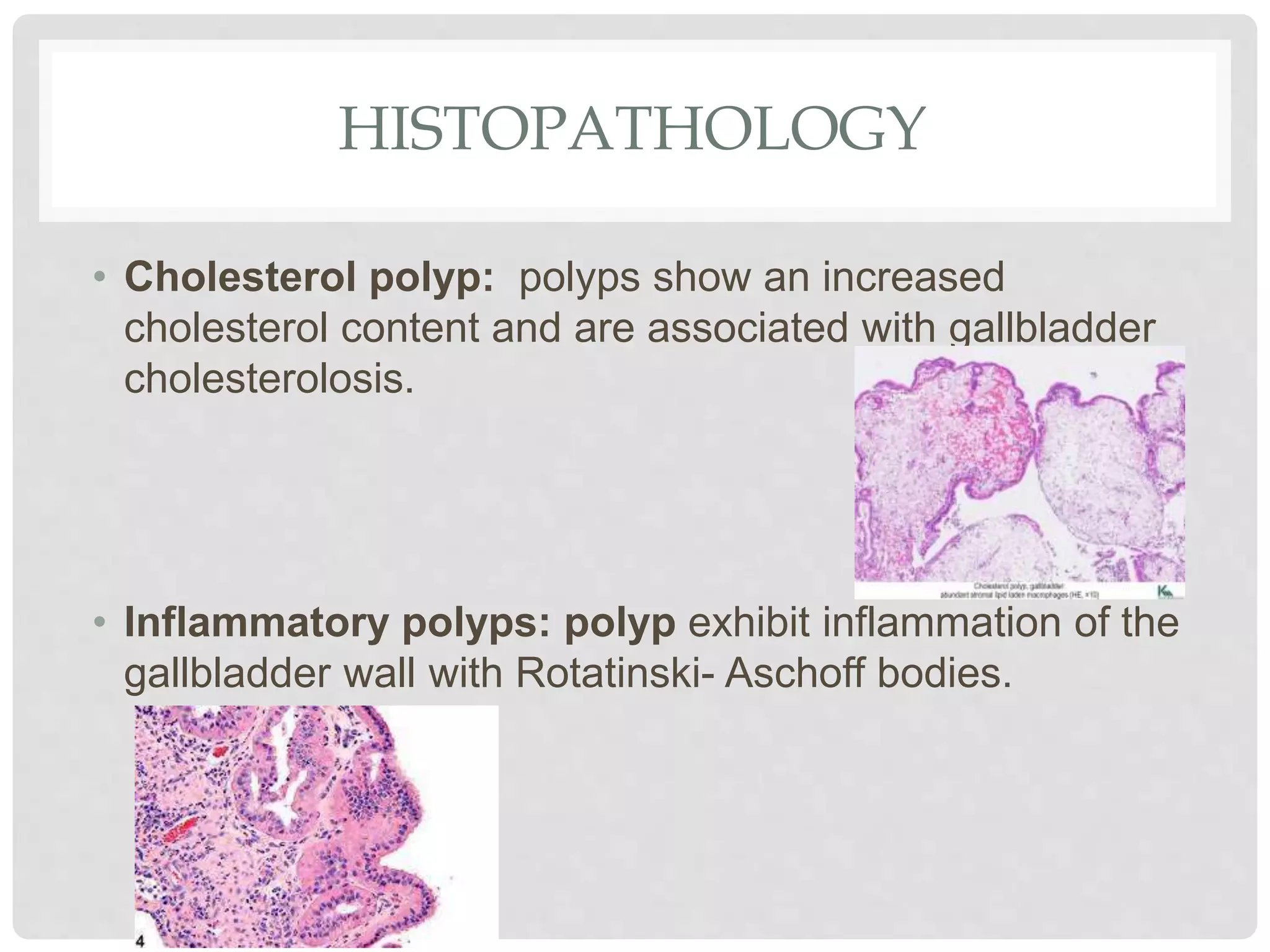
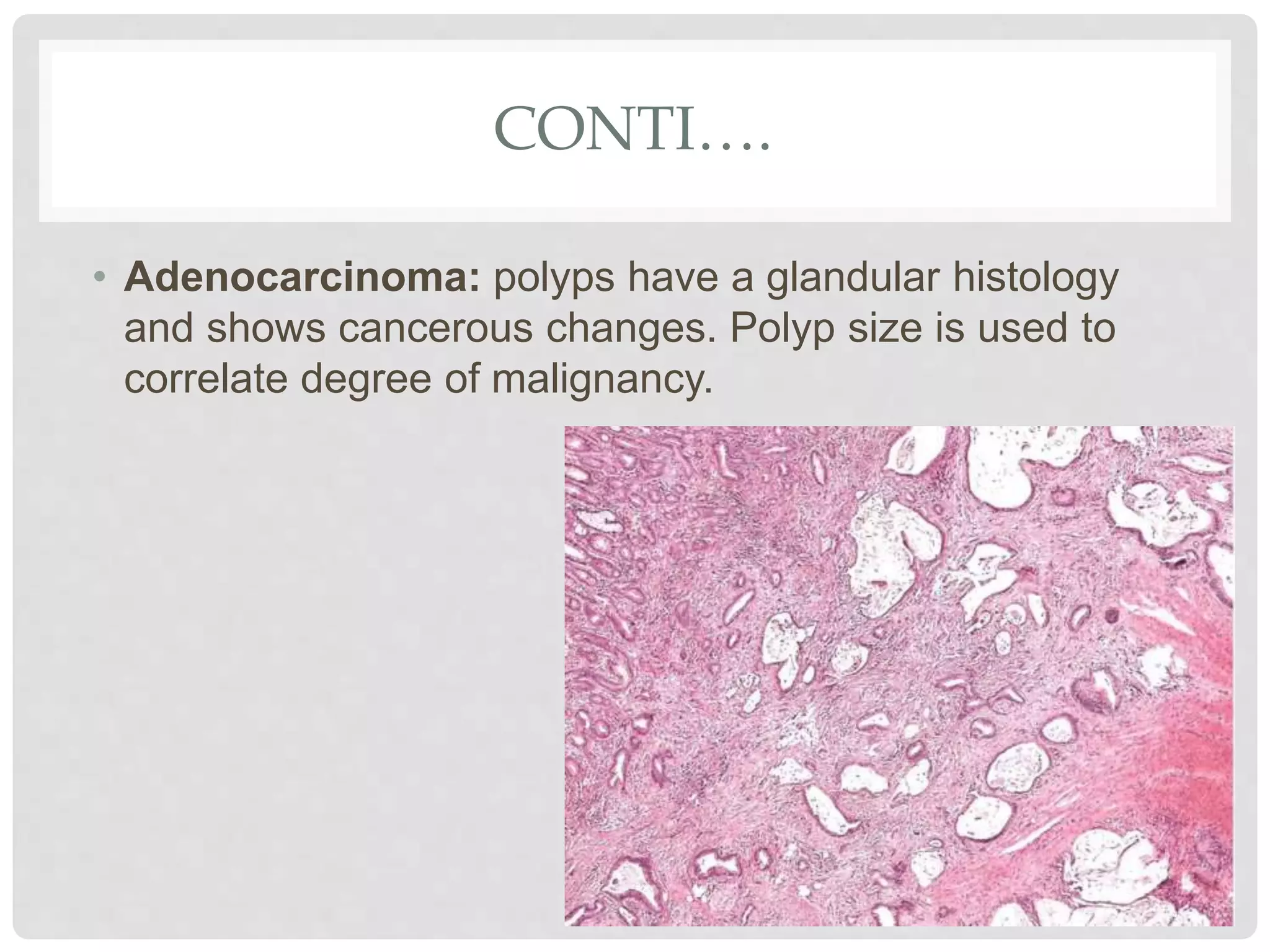
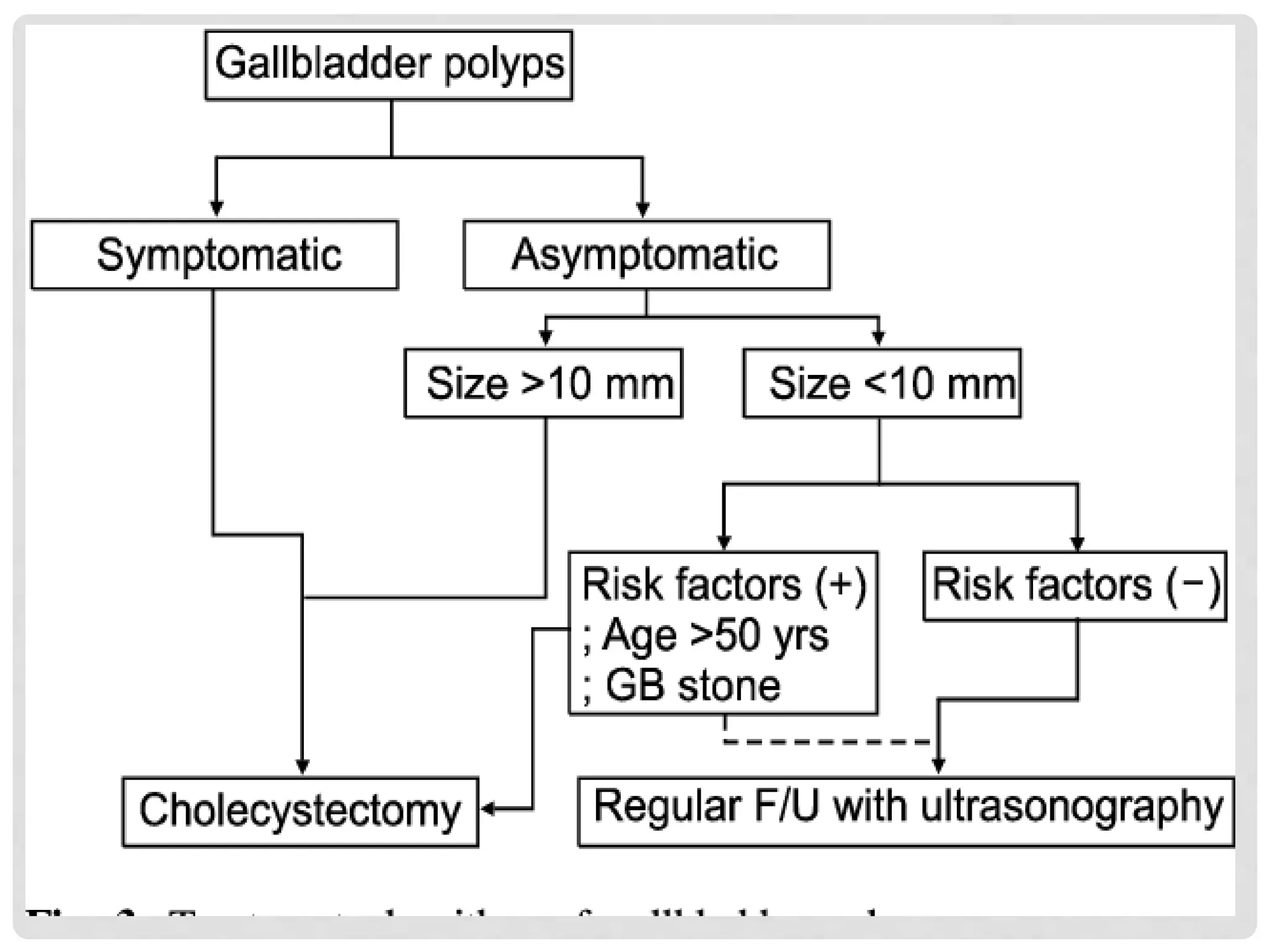
Gallbladder polyps are abnormal growths that can develop on the lining of the gallbladder. While most gallbladder polyps are non-cancerous, some polyps have the potential to become malignant. The document discusses the epidemiology, classification, pathology, diagnosis, and management of gallbladder polyps. Polyps larger than 10mm or those demonstrating changes in size have a higher risk of cancer and often require surgical removal of the gallbladder.