
Downloaded 19 times
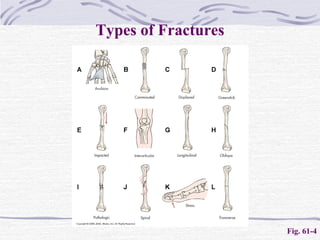
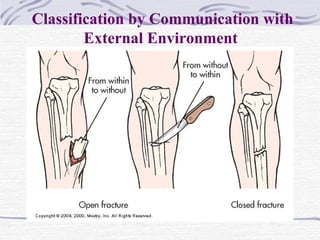
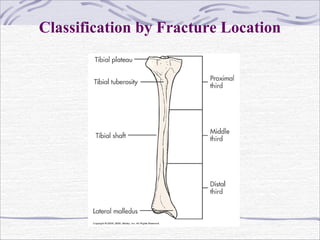


Fractures are breaks in the continuity of bone that are usually caused by trauma. They are described and classified based on their type, communication with the external environment, and anatomic location. The goals of treatment are to realign bone fragments through reduction, immobilize the bones to maintain alignment through fixation methods like casting, and restore normal function. Complications can include infection, compartment syndrome, venous thrombosis, fat embolism syndrome, malunion, non-union, osteomyelitis, avascular necrosis, and shortening.























































































