Downloaded 259 times
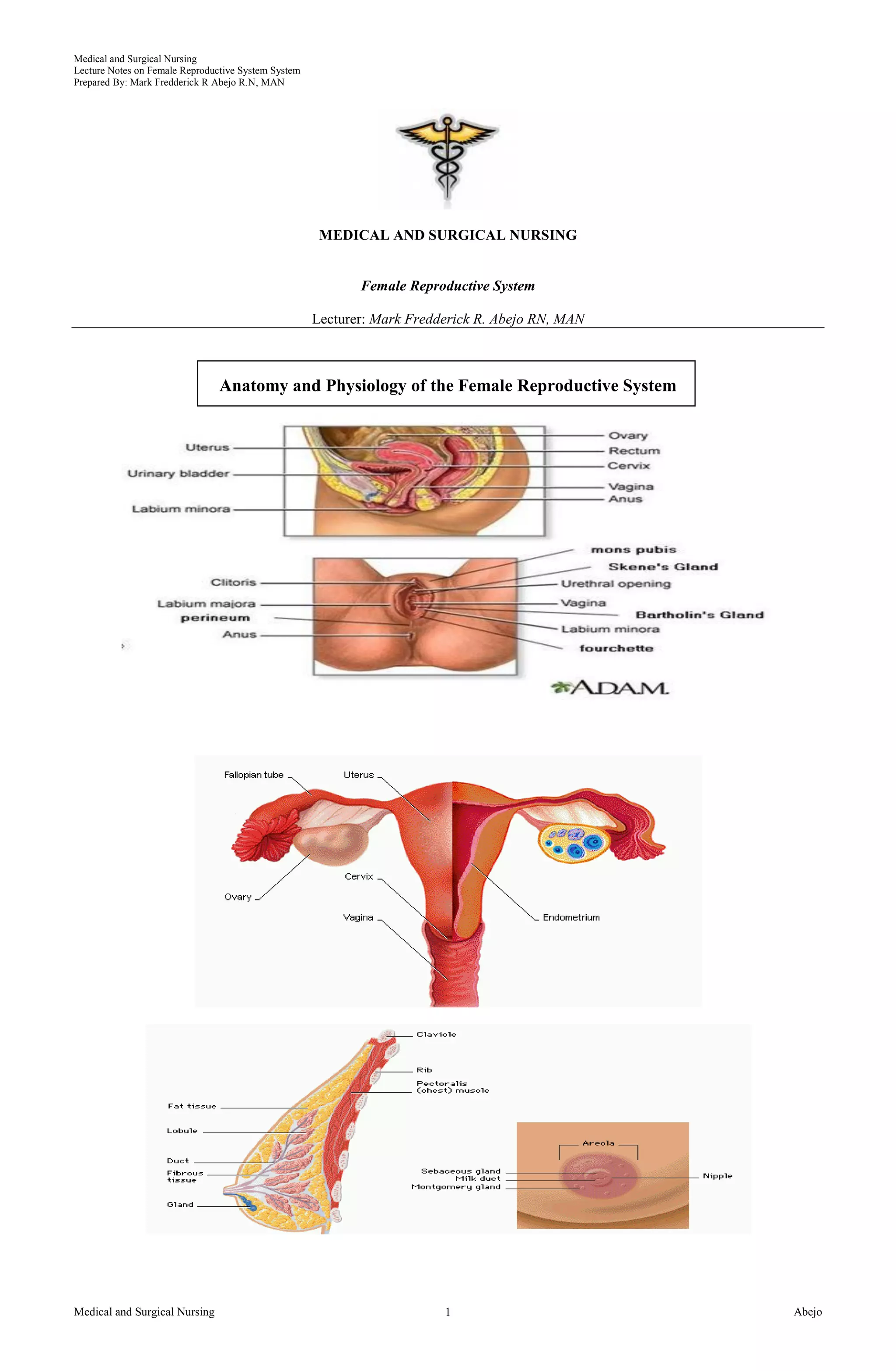






This document provides notes on the female reproductive system prepared by Mark Fredderick R. Abejo. It describes the internal and external female reproductive organs including the vagina, cervix, uterus, fallopian tubes, ovaries, vulva, and clitoris. It also discusses common female reproductive disorders such as ovarian cysts, endometriosis, and uterine fibroids/leiomyomas. The causes, risk factors, clinical manifestations, diagnostic tests, and collaborative management of each condition are described.









































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)






![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)






