




































































































































![References:
[1] Case-Smith, J. (2001). Occupational
therapy for children. St. Louis Missouri, USA:
Mosby, Inc.
[2] Solomon, J. (2006). Pediatric skills for
occupational therapy assistants. St. Louis
Missouri, USA: Mosby, Inc.
[3] Wagenfeld, A. (2005). Foundations of
pediatric practice for occupational therapy
assistants. USA: SLACK Inc.](https://image.slidesharecdn.com/feeding-qld-130605175223-phpapp02/85/Feeding-152-320.jpg)


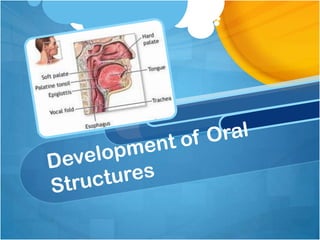
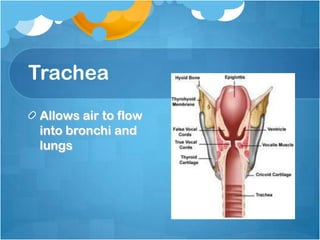
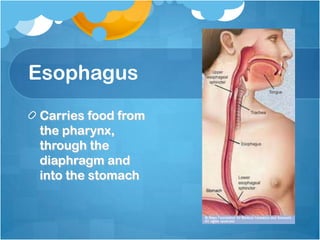
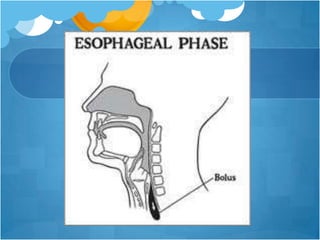
The document addresses the anatomy, physiology, and developmental skills related to feeding in infants and children, focusing on dysphagia and associated feeding problems. It outlines phases of swallowing, the importance of oral structure function, sensory processing issues, and intervention strategies for feeding difficulties. The comprehensive analysis includes assessment methods, treatment programs, and adaptations for children with various medical conditions affecting feeding, emphasizing the role of a multi-disciplinary feeding team.



















































































