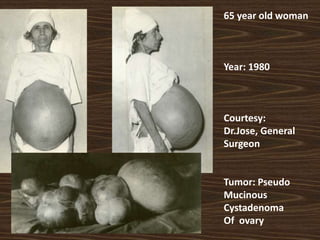
1) Ovarian cysts are common in premenopausal women and are usually benign, with a risk of malignancy around 1 in 1000. Postmenopausal cysts require more evaluation due to higher risk of cancer.
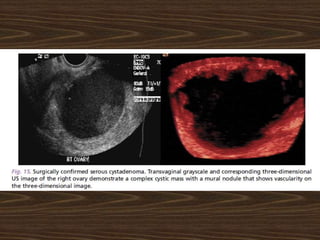
2) Conservative management is recommended for small, unilateral, simple cysts in premenopausal women, with follow up ultrasound. Suspicious cysts based on features like size, complexity, CA125 levels should be referred to specialists.
3) Serial ultrasound can monitor simple, thin-walled cysts under 10cm in postmenopausal women, which often resolve spontaneously. But thicker-walled or larger cysts require further evaluation due to higher cancer risk.


![CA- 125
• Raised in > 80 % ovarian cancers
greater than 200 U per mL [200 kU per L] in premenopausal
women and
greater than 35 U per mL [35 kU per L]
in postmenopausal women
positive predictive value
49 % in premenopausal women
98 % in postmenopausal women.
• But raised in only 50 % Stage 1
• Also raised in benign conditions and other malignancies](https://image.slidesharecdn.com/ovariancystinperimenopausenagpur-180323115932/85/Ovarian-cyst-in-perimenopause-12-320.jpg)























































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)











![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)



