Download to read offline


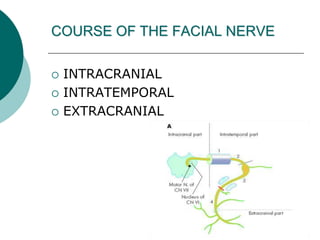

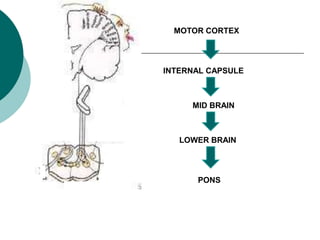




















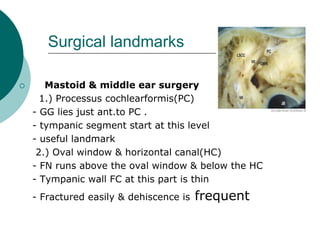









































The document discusses the facial nerve, including its anatomy and course from the brainstem through the temporal bone. It describes the intratemporal, intracanalicular, and extracranial segments. Disorders of the facial nerve are also reviewed, such as Bell's palsy caused by viral infections, tumors, trauma, or complications from ear infections. Surgical landmarks, testing, classification systems, pathology of nerve injuries, and potential complications of regeneration like synkinesis are summarized. Congenital causes, infections, tumors, and other neurological or miscellaneous etiologies of facial palsy are outlined.