Facial nerve seminar
•Download as PPTX, PDF•
2 likes•103 views

The document provides information on the facial nerve (cranial nerve VII), including its embryology, nuclei, course, branches, landmarks, neurophysiology, causes of damage, and grading systems for facial palsy. It describes the facial nerve's development during gestation, its motor, sensory and parasympathetic functions. Key points along its intra- and extracranial course are identified. Variations, injuries, and resulting functional deficits are also discussed.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Facial nerve seminar
Similar to Facial nerve seminar (20)
More from Jeff Zacharia
Recently uploaded
Recently uploaded (20)
Facial nerve seminar
- 1. FACIAL NERVE DR. JEFF K. ZACHARIA 1ST YEAR POST GRADUATE DEPARTMENT OF ORAL & MAXILLOFACIAL SURGERY A.J. INSTITUTE OF DENTAL SCIENCES
- 2. CONTENTS • INTRODUCTION • EMBRYOLOGY • NUCLEI • COURSE AND RELATIONS • LANDMARKS • NEUROPHYSIOLOGY • CAUSES OF FACIAL PALSY • TESTING OF FACIAL NERVE • BELL’S PALSY • CONCLUSION • REFERENCES
- 3. INTRODUCTION • THE FACIAL NERVE IS THE VII CRANIAL NERVE. • IT IS THE NERVE OF THE SECOND BRANCHIAL ARCH.
- 4. EMBRYOLOGY MAIN PATTERN OF THE NERVE’S COMPLEX COURSE, BRANCHING PATTERN AND RELATIONSHIPS ARE ESTABLISHED DURING THE FIRST THREE MONTHS OF PRENATAL LIFE. DURING THIS PERIOD, THE MUSCLES OF EXPRESSION DIFFERENTIATE, BECOME FUNCTIONAL AND ACTIVELY CONTRACT. IMPORTANT STEPS IN FACIAL NERVE DEVELOPMENT OCCUR THROUGH OUT GESTATION AND THE NERVE IS NOT FULLY DEVELOPED UNTIL 4 YEARS
- 5. TIME DURING GESTATION THAT ANATOMICAL STRUCTURES APPEAR • 3RD WEEK: FACIOACOUSTIC MEATUS DEVELOPS • 4TH WEEK: FACIAL NERVE DIVIDES INTO TWO PARTS • 5TH WEEK: GENICULATE GANGLION, NERVUS INTERMEDIUS, GREATER PETROSAL NERVE VISIBLE • 7TH & 8TH WEEK: MUSCLES OF FACIAL EXPRESSION DEVELOP • 11TH WEEK: FACIAL NERVE ARBORIZED.
- 6. NUCLEI • THE FIBRES OF THE NERVE ARISE FROM 4 NUCLEI SITUATED AT LOWER PONS: 1. BRACHIAL NUCLEUS (MOTOR NUCLEUS) 2. SUPERIOR SALIVATORY NUCLEUS (PARASYMPATHETIC NUCLEUS) 3. NUCLEUS OF TRACTUS SOLITARIUS (TASTE) 4. SPINAL TRIGEMINAL NUCLEUS (GENERAL SENSATION)
- 7. IT IS A MIXED NERVE MOTOR: MUSCLES OF EXPRESSION, STYLOHYOID MUSCLE, POSTERIOR BELLY OF DIGASTRIC AND STAPEDIUS MUSCLE. PARASYMPATHETIC: SUBMANDIBULAR GLAND, SUBLINGUAL GLAND, NASAL GLANDS, PALATINE GLANDS AND LACRIMAL GLANDS. SPECIAL SENSORY: TASTE FROM ANTERIOR 2/3RD OF THE TONGUE. SENSORY: SKIN AROUND THE EAR
- 8. BRACHIMOTOR NUCLEUS IT IS DIVIDED INTO AN UPPER PART AND A LOWER PART THE UPPER PART IS CONTROLLED BY THE LEFT AND THE RIGHT SIDE OF THE BRAIN. THE UPPER PART OF THE NUCLEUS IS RESPONSIBLE FOR SUPPLYING THE MUSCLES OF THE UPPER PART OF THE FACE (ORBICULARIS OCULI, FRONTALIS MUSCLE, CORRUGATOR SUPERCILI, NASALIS, LEVATOR LABII SUPERIORIS) THE LOWER PART OF THE NUCLEUS IS CONTROLLED BY THE OPPOSITE OF
- 9. COURSE AND RELATIONS OF FACIAL NERVE
- 10. COURSE AND RELATIONS THE COURSE OF THE FACIAL NERVE IS VERY COMPLEX SINCE THERE ARE MANY BRANCHES. THE COURSE CAN BE DIVIDED INTO THREE PARTS: INTRACRANIAL INTRATEMPORAL EXTRACRANIAL
- 11. INTRACRANIAL COURSE THE NERVE ARISES IN THE PONS, AN AREA OF THE BRAINSTEM. IT BEGINS AS TWO ROOTS: A LARGE MOTOR ROOT AND A SMALL SENSORY ROOT THE TWO ROOTS TRAVEL THROUGH THE INTERNAL ACOUSTIC MEATUS, A 1CM LONG OPENING IN THE PETROUS PART OF THE TEMPORAL BONE WHERE THEY ARE IN VERY CLOSE PROXIMITY TO THE INNER EAR. IT TRAVELS SLIGHTLY ABOVE AND TH
- 12. INTRATEMPORAL COURSE THE TOTAL LENGTH OF THE NERVE HERE IS 22-33 MM
- 13. INTRATEMPORAL BRANCHES NERVE TO STAPEDIUS: ARISES FROM THE MASTOID SEGMENT AND SUPPLIES THE STAPEDIUS MUSCLE. CHORDA TYMPANI: ARISES FROM THE MASTOID SEGMENT, MOVES ANTERIORLY BETWEEN INCUS & MALLEUS AND JOINS THE LINGUAL NERVE TO SUPPLY THE ANTERIOR 2/3RD OF THE TONGUE. IT ALSO SUPPLIES PARASYMPATHETIC FIBRES TO SUBMANDIBULAR AND SUBLINGUAL GLANDS. SENSORY FIBRES: JOINS THE AURICULAR BRANCH OF VAGUS
- 14. MORPHOLOGIC PECULIARITIES (GERRIER 1977) a) INDIVIDUAL SHEATH OF PIA MATER CURVES UP AND CONTINUES WITH ARACHINOID. b) SLIGHT CONSTRICTION OF THE NERVE JUST PRIOR TO THE LABYRINTH SEGMENT WHICH IS A NORMAL CONSTRICTION. c) CHANGE IN THE DIRECTION OF THE NERVE THAT PRODUCES AN ANGLE OF 132°
- 15. THE NERVE THEN EMERGES OUT OF THE STYLOMASTOID FORAMEN IN A NEWBORN, THE STYLOMASTOID FORAMEN IS AT A HIGHER LEVEL WITH THE FACIAL NERVE EMERGING AT THE LEVEL OF THE MASTOID ANTRUM
- 16. EXTRACRANIAL COURSE AFTER EXITING THE FORAMEN, IT GIVES RISE TO THE: POSTERIOR AURICULAR NERVE: WHICH ASCENDS IN FRONT OF THE MASTOID PROCESS AND PROVIDES MOTOR INNERVATION TO THE INTRINSIC AND EXTRINSIC MUSCLES OF THE OUTER EAR. IT ALSO SUPPLIES THE OCCIPITAL PART OF THE OCCIPITOFRONTALIS MUSCLE. NERVE TO THE POSTERIOR BELLY OF THE DIGASTRIC MUSCLE: INNERVATES THE POSTERIOR BELLY OF THE DIGASTRIC MUSCLE WHICH IS RESPONSIBLE FOR RAISING THE HYOID BONE. NERVE TO THE STYLOHYOID MUSCLE: INNERVATES THE STYLOHYOID MUSCLE WHICH IS RESPONSIBLE FOR RAISING THE HYOID BONE.
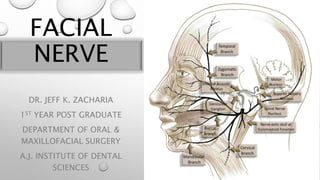
- 17. THE MAIN TRUNK OF THE NERVE CONTINUES ANTERIORLY AND INFERIORLY INTO THE PAROTID GLAND AND TERMINATES BY SPLITTING INTO FIVE BRANCHES: TEMPORAL BRANCH: INNERVATES THE FRONTALIS, ORBICULARIS OCULI AND CORRUGATOR SUPERCILII ZYGOMATIC BRANCH: INNERVATES THE ORBICULARIS OCULI. BUCCAL BRANCH: INNERVATES THE ORBICULARIS ORIS, BUCCINATOR AND ZYGOMATICUS MUSCLES. MARGINAL MANDIBULAR BRANCH: INNERVATES THE MENTALIS MUSCLE. CERVICAL BRANCH: INNERVATES THE PLATYSMA
- 18. SUMMARY OF BRANCHES OF FACIAL NERVE A: WITHIN THE FACIAL CANAL: 1. GREATER PETROSAL NERVE 2. NERVE TO STAPEDIUS 3. THE CHORDA TYMPANI
- 19. B: AT ITS EXIT FROM STYLOMASTOID FORAMEN 1. POSTERIOR AURICULAR NERVE 2. DIGASTRIC 3. STYLOHYOID
- 20. C: TERMINAL BRANCHES WITHIN THE PAROTID GLAND 1. TEMPORAL 2. ZYGOMATIC 3. BUCCAL 4. MARGINAL MANDIBULAR 5. CERVICAL
- 21. VASCULAR SUPPLY THE FACIAL NERVE GETS IT’S BLOOD SUPPLY FROM: 1. ANTERIOR INFERIOR CEREBELLAR ARTERY – AT THE CEREBELLOPONTINE ANGLE 2. LABYRINTHINE ARTERY (BRANCH OF ANTERIOR INFERIOR CEREBELLAR ARTERY) – WITHIN INTERNAL ACOUSTIC MEATUS 3. SUPERFICIAL PETROSAL ARTERY (BRANCH OF MIDDLE MENINGEAL ARTERY) – GENICULATE GANGLION AND NEARBY PARTS
- 22. 4. STYLOMASTOID ARTERY (BRANCH OF POSTERIOR AURICULAR ARTERY) – MASTOID SEGMENT 5. POSTERIOR AURICULAR ARTERY SUPPLIES THE FACIAL NERVE DISTAL TO STYLOMASTOID FORAMEN. 6. VENOUS DRAINAGE PARALLELS THE ARTERIAL BLOOD SUPPLY
- 23. LANDMARKS OF FACIAL NERVE
- 24. LANDMARKS FOR EXTRATEMPORAL PART TRAGAL POINTER OF CONLEY: THE NERVE IS LOCATED MEDIAL AND ABOUT 1 CM INFERIOR TO THE TRAGAL CARTILAGE TYMPANOMASTOID SUTURE: THIS IS LOCATED AT THE APEX OF THE VAGINO-MASTOID ANGLE OR VALLEY OF THE NERVE . THE FACIAL NERVE RUNS DEEP TO THIS SUTURE.
- 25. STYLOID PROCESS: THE NERVE PASSES LATERAL TO THE STYLOID. TENDON OF POSTERIOR BELLY OF DIGASTRIC MUSCLE: THE MAIN TRUNK OF THE NERVE CAN BE FOUND MIDWAY BETWEEN THE CARTILAGINOUS POINTER OF THE EXTERNAL ACCOUSTIC MEATUS AND THE POSTERIOR BELLY OF DIGASTRIC MUSCLE. POSTERIOR AURICULAR VEIN OR THE RETROMANDIBULAR VEIN
- 26. LANDMARKS IN THE MASTOID AND MIDDLE EAR THE COG: IT IS A BONY RIDGE WHICH HANGS FROM THE TEGMEN, ANTERIOR TO THE HEAD OF THE MALLEUS AND IS USEFUL FOR IDENTIFYING THE FIRST GENU COCHLEARIFORM PROCESS: IT IS INFERIOR TO THE ANTERIOR PORTION OF THE TYMPANIC SEGMENT OF THE FACIAL NERVE.
- 27. OVAL WINDOW: IT IS A USEFUL GUIDE TO THE POSTERIOR PORTION OF THE HORIZONTAL SEGMENT OF THE NERVE. THE NERVE LIES ABOVE THE OVAL WINDOW LATERAL SEMICIRCULAR CANAL: IT LIES POSTERIOR- SUPERIOR TO THE SECOND GENU AND IS A CONSTANT LANDMARK. RETROFACIAL AIR CELLS: IT HELPS IN DELINEATING THE MEDIAL ASPECT OF THE VERTICAL SEGMENT OF THE FACIAL NERVE.
- 28. LANDMARKS IN THE MIDDLE CRANIAL FOSSA THE GREATER PETROSAL NERVE IS IDENTIFIED AND FOLLOWED BACKWARDS TO THE GENICUALATE GANGLION AND FACIAL NERVE IS IDENTIFIED. IDENTIFICATION OF THE INTERNAL AUDITORY CANAL SINCE IT LIES IN THE SAME CORONAL PLANE WITH THE EXTERNAL AUDITORY CANAL. THE BULGE OF THE SEMICIRCULAR CANAL CAN BE IDENTIFIED AND SUBSEQUENTLY THE INTERNAL AUDITORY CANAL IS IDENTIFIED.
- 29. VARIATIONS IN FACIAL NERVE
- 30. • VARIATION 1: FACIAL NERVE GOES ABOVE THE LATERAL SEMICIRCULAR CANAL • VARIATION 2: FACIAL NERVE GOES ABOVE THE FOOT PLATE OF STAPES • VARIATION 3: GOES IN BETWEEN THE COURA OF THE STAPES. VARIATIONS IN TYMPANIC SEGMENT
- 31. • VARIATION 4: GOES INFERIOR TO THE FOOT PLATE OF STAPES • VARIATION 5: GOES IN BETWEEN THE OVAL WINDOW & ROUND WINDOW • VARIATION 6: GOES BELOW ROUND WINDOW • VARIATION 7: NERVE SPLITS
- 32. VARIATIONS IN MASTOID SEGMENT • VARIATION 1: (DORSAL HUMP): HUMPS BELOW LATERAL SEMICIRCULAR CANAL • VARIATION 2: CURVES ANTERIORLY AND CONTINUES ABOVE THE FOOT PLATE • VARIATION 3: VERTICAL PART OF THE NERVE
- 33. • VARIATION 4: VERTICAL PART OF THE FACIAL NERVE GOES VERY POSTERIORLY AND STAYS ABOVE THE SIGMOID SINUS • VARIATION 5: BIFURCATION OR TRIFURCATION • VARIATION 6: HYPOPLASIA OF VERTICAL PART OF FACIAL NERVE
- 34. NEUROPHYSIOLOGY OF FACIAL NERVE
- 35. NEUROPHYSIOLOGY OF FACIAL NERVE FACIAL EXPRESSION DEPENDS ON 7000 MOTOR FIBRES OF THE FACIAL NERVE FIRING IN UNISON TO BRING ABOUT MUSCULAR CONTRACTION
- 36. DEGREES OF NERVE INJURY SEDDON (1943) DESCRIBED THREE TYPES OF NERVE INJURY: NEUROPRAXIA: PRESSURE ON A PERIPHERAL NERVE CAN BLOCK THE TRANSMISSION OF THE IMPULSES WITHOUT DEATH AND DEGENERATION OF THE AXON BEYOND THE SITE OF PRESSURE. ASSOCIATED WITH LOSS OF MYELIN. THIS IS A REVERSIBLE CONDUCTION BLOCK. AXONTEMESIS: SECTIONING OF AN AXON AND RESULTS IN DEATH OF THE BLOCKED DISTAL SEGMENT. NEURONTEMESIS: SECTIONING OF THE ENTIRE NERVE TRUNK
- 37. SUNDERLAND (1978) CLASSIFIED NERVE INJURIES INTO 5 DEGREES. FIRST DEGREE: INDICATES COMPRESSION OF THE NERVE. IT IS REVERSIBLE. SECOND DEGREE: THERE IS INTERRUPTION OF THE AXON AND MYELIN. OCCURS WHEN THE COMPRESSION PERSISTS. HERE, THERE IS LOSS OF AXON BUT ENDONEURIUM IS INTACT. RECOVERY MAY TAKE MORE THAN 1 – 2 MONTHS. THIRD DEGREE: THERE IS LOSS OF MYELIN TUBES DUE TO INCREASED INTRANEURAL PRESSURE. RECOVERY TAKES ABOUT 2 – 4 MONTHS. THERE MAY NOT BE COMPLETE RECOVERY FOURTH DEGREE: PARTIAL TRANSECTION OF THE NERVE. RECOVERY IS POOR.
- 38. HOUSE AND BRACKMAN FACIAL NERVE GRADING SYSTEM APPROVED BY AMERICAN ACADEMY OF OTOLARYNGOLOGY GRADE I: NORMAL GRADE II: MILD DYSFUNCTION FOREHEAD MOTION IS MODERATE TO GOOD. SLIGHT ASYMMETRY OF THE MOUTH. EYE CLOSURE COMPLETE GRADE III: MODERATE DYSFUNCTION FOREHEAD MOTION IS SLIGHT TO MODERATE. WEAKNESS OF ANGLE OF THE MOUTH ON MAXIMAL EFFORT EYE CLOSURE IS INCOMPLETE WITH MAXIMAL EFFORT
- 39. GRADE IV: MODERATELY SEVERE DYSFUNCTION NO FOREHEAD MOTION MOUTH MOVEMENT IS COMPLETE ON MAXIMAL EFFORT EYE CLOSURE IS INCOMPLETE WITH MAXIMAL EFFORT GRADE V: SEVERE DYSFUNCTION NO FOREHEAD MOTION VERY SLIGHT MOUTH MOVEMENT EYE CLOSURE IS INCOMPLETE GRADE VI: TOTAL PARALYSIS
- 40. DAMAGE TO THE FACIAL NERVE
- 41. DAMAGE TO THE FACIAL NERVE THE FACIAL NERVE HAS A WIDE RANGE OF FUNCTIONS. THUS, DAMAGE TO THE NERVE CAN PRODUCE A VARIED SET OF SYMPTOMS, DEPENDING ON THE SITE OF THE LESION.
- 42. INTRACRANIAL LESIONS • THE MUSCLES OF FACIAL EXPRESSION WILL BE PARALYZED OR SEVERELY WEAKENED. • CHORDA TYMPANI – REDUCED SALIVATION AND LOSS OF TASTE ON THE IPSILATERAL 2/3 OF THE TONGUE. • NERVE TO STAPEDIUS – IPSILATERAL HYPERACUSIS (HYPERSENSITIVE TO SOUND). • GREATER PETROSAL NERVE – IPSILATERAL REDUCED LACRIMAL FLUID PRODUCTION.
- 43. EXTRACRANIAL LESIONS • PAROTID GLAND PATHOLOGY – E.G. A TUMOR, PAROTITIS, SURGERY. • INFECTION OF THE NERVE – PARTICULARLY BY THE HERPES VIRUS. • COMPRESSION DURING FORCEPS DELIVERY – THE NEONATAL MASTOID PROCESS IS NOT FULLY DEVELOPED, AND DOES NOT PROVIDE COMPLETE PROTECTION OF THE NERVE.
- 44. CAUSES OF FACIAL PALSY
- 45. CAUSES OF FACIAL PALSY AT BIRTH • FORCEPS DELIVERY • MOEBIUS SYNDROME • DYSTROPHIA MYOTONICA TRAUMA A) ACCIDENTAL • SKULL BASE FRACTURES • PENETRATING INJURY TO MIDDLE EAR • BAROTRAUMA • SCUBA DIVING B) IATROGENIC • MASTOID SURGERY • PAROTID SURGERY • POSTAURAL LOCAL Infections A) Bacterial • Otitis media • Tuberculosis • Botulism • Lyme disease B) Viral • Ramsay Hunt Syndrome • Poliomyelitis C) Fungal • Mucormycosis Neoplastic • Vestibular schwannoma • Von Recklinghausen’s disease • Teratoma • Leukemia Neurological • Multiple sclerosis • Myasthemis gravis • Encephalitis Miscellaneous A) Toxic • Tetanus • Diphteria B)Metabolic • Diabetes
- 46. TESTING THE FACIAL NERVE
- 47. SCHIRMER’S TEST • A STRIP OF PAPER OF 5 CM X 0.5 CM IS PLACED ON THE LOWER CONJUNCTIVAL FORNIX OF EACH EYE AND THE PATIENT IS INTRODUCED TO INHALATION AMMONIA TO ENHANCE LACRIMATION. • A REDUCED LACRIMATION BY 30% COMPARED TO THE NORMAL SIDE IS SIGNIFICANT. SALIVARY FLOW TEST • A NO. 50/60 POLYETHYLENE CATHETER IS INTRODUCED TO BOTH WHARTON’S PAPILLAE FOR ABOUT 3 MM. • THE PATIENT IS GIVEN A FEW DROPS OF LEMON, AND THE NUMBER OF DROPS OF SALIVA OVER ONE TO FIVE MINUTES IS MONITORED. • A 25% REDUCTION BETWEEN THE SIDES IS SIGNIFICANT
- 48. TASTE SENSATION OF THE ANTERIOR 2/3RD OF THE TONGUE • IT IS BEST ASSESSED USING A ELECTROGUSTOMETRY, HOWEVER, IT IS NOT PROVED TO BE A USEFUL DIAGNOSTIC TOOL. STAPEDIAL REFLEX • THIS TEST ASSESSES THE STAPEDIAL MOVEMENTS BY TYMPANOMETRY. NERVE CONDUCTION TIME • IT IS USED TO TEST THE LATENCY RESPONSE OF A MUSCLE (INNERVATED BY FACIAL NERVE) ON ELECTRICAL STIMULATION. NERVE EXCITABILITY TEST • PERFORMED BY STIMULATING THE NERVE AT THE STYLOMASTOID FORAMEN AND IS DETERMINED BY A TWITCH RESPONSE IN THE FACIAL MUSCULATURE. BLINK TEST • THIS TEST IS DONE BY ELECTRICALLY STIMULATING THE NERVE AT THE SUPRAORBITAL FORAMEN.
- 49. OTHER TESTS INCLUDE: ELECTROMYOGRAPHY MAXIMAL STIMULATION TEST ELECTRONEUROGRAPHY MAGNETIC STIMULATION
- 50. BELL’S PALSY
- 51. BELL’S PALSY DESCRIBED BY SIR CHARLES BELL (1829) IT IS AN ACUTE IDIOPATHIC LOWER MOTOR NEURON PALSY OF THE FACIAL NERVE THAT IS UNILATERAL, SELF LIMITING, NON- PROGRESSIVE, NON LIFE THREATENING AND SPONTANEOUSLY REMITS BY 4-6 MONTHS AND ALWAYS BY 1 YEAR.
- 52. THEORIES VASCULAR ISCHEMIC THEORY IN THIS THEORY, THERE IS DECREASE IN CIRCULATION TO THE FACIAL NERVE WHICH IS BELIEVED TO BE DUE TO THE INTERRUPTION OF A NUTRIENT VESSEL. VIRAL THEORY IT IS CONCLUDED THAT BELL’S PALSY IS AN ACUTE BENIGN CRANIAL POLYNEURITIS CAUSED BY THE REACTIVATION OF HERPES SIMPLEX VIRUS. THE VIRUS REPLICATES IN THE GANGLION CELLS CAUSING LOCAL DAMAGE AND HYPOFUNCTION OF THE NERVES THEREFORE PREVENTING
- 53. HEREDITARY THEORY A FAMILIAL ANATOMIC VARIATION IN THE FACIAL CANAL (BONY CONSTRICTION) MAY ACCOUNT FOR A GREATER TENDENCY TOWARDS THE DEVELOPMENT OF FACIAL PALSY. IT IS BELIEVED TO BE A RECESSIVE TRAIT.
- 54. EXAMINATION DIFFERENTIATE BETWEEN UPPER MOTOR LESION (UML) OR LOWER MOTOR MOTOR NEURON LESION (LML) IN UML, THE FRONTALIS MUSCLE IS SPARED ALLOWING NORMAL FURROWING OF EYE BROW AND EYE BLINKING. IN LML, ALL THE MUSCLES OF FACIAL EXPRESSION ARE AFFECTED ON ONE SIDE. EYE CLOSURE (ORBICULARIS OCULI) WIDE SMILE BLOWING (BUCCINATOR, ORBICULARIS ORIS)
- 55. CLINICAL FEATURES • RAPID ONSET OF MILD WEAKNESS TO TOTAL PARALYSIS ON ONE SIDE OF THE FACE. • FACIAL DROOP AND DIFFICULTY IN MAKING EXPRESSIONS. • INCREASED SENSITIVITY TO SOUND. • DECREASED ABILITY TO TASTE. • DRIPPING OF SALIVA (WEIR, PENTLAND & MURRAY, 1993) • ACCUMULATION OF FOOD INSIDE THE CHEEK. • PAIN AROUND THE JAW AND/OR BEHIND EAR OF THE AFFECTED SIDE. • FLATTENING OF THE NASOLABIAL FOLD.
- 56. MANAGEMENT MEDICAL MANAGEMENT PREDNISOLONE 1MG/KG/DAY OR 60 MG GIVEN ORALLY ACYCLOVIR 200 TO 400 MG GIVEN ORALLY VASODILATORS LIKE XANITOL ASCORBIC ACID MULTIVITAMINS LIKE B1, B6 AND B12 SURGICAL TREATMENT FACIAL NERVE DECOMPRESSION IN CASE OF NO IMPROVEMENT AFTER 3 WEEKS OF MEDICAL TREATMENT.
- 57. CONCLUSION SURGEONS HAVE TO PAY ATTENTION TO MINIMIZE THE RISK OF COMPLICATION DURING PAROTIDECTOMY. THE BEST WAY TO REDUCE IATROGENIC FACIAL NERVE INJURY IS TO HAVE A CLEAR UNDERSTANDING OF THE ANATOMY, GOOD SURGICAL TECHNIQUE AND USE OF MULTIPLE LANDMARKS. THE PATIENT HAS TO BE INFORMED ABOUT THE COSMETIC SEQUELAE OF THE INCISION AND ALL PATIENTS HAVE TO BE TOLD THAT FACIAL NERVE PARALYSIS IS POSSIBLE AND CAN BE PARTIAL OR TOTAL, TEMPORARY OR PERMANENT.
- 58. REFERENCES B.D. CHAURASIA’S HUMAN ANATOMY VOLUME III ATLAS OF FACIAL NERVE SURGERY EDITION II
- 59. THANK YOU
Editor's Notes
- Immediately distal to this, motor branches are sent to the posterior belly of the digastric muscle and to the stylohyoidmuscle.
- parotid gland is innervated by the glossopharyngeal nerve).
- The term facial palsy generally refers to weakness of the facial muscles, mainly resulting from temporary or permanent damage to the facial nerve
- In this theory, there is decrease in circulation to the facial nerve which is believed to be due to the interruption of a nutrient vessel which could be due to compression of the facial nerve in the facial canal or due to presence of a thickened fibrous sheath.