Downloaded 78 times





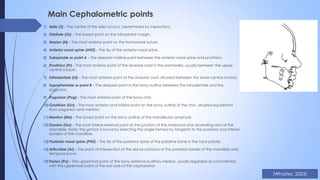





Cephalometry is a standardized form of skull radiography used in orthodontics to assess the relationship between teeth, jaws, and facial skeleton. It is important for initial diagnosis, treatment planning, monitoring treatment progress, and orthognathic surgery. A cephalostat machine is used to position and stabilize the patient's head while lateral or posteroanterior radiographs are taken. Key cephalometric planes and landmarks are identified on the radiographs to evaluate skeletal and dental relationships.



































































