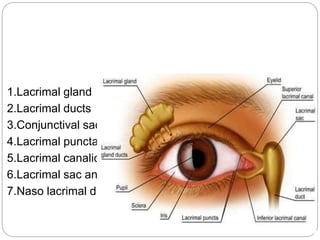
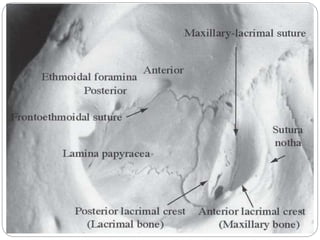
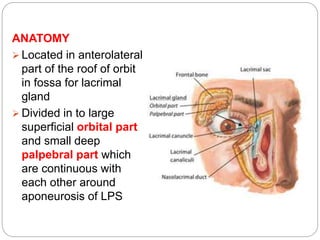
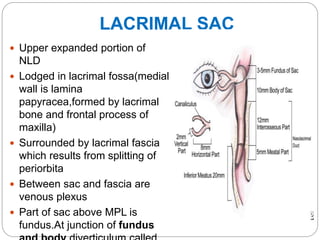
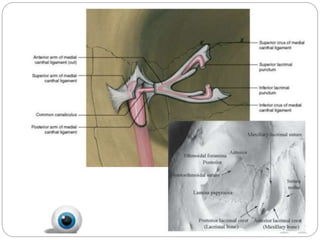
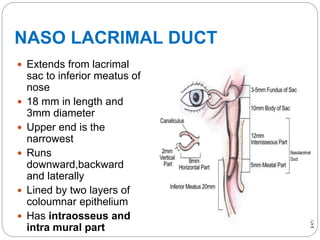

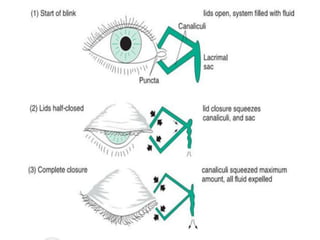
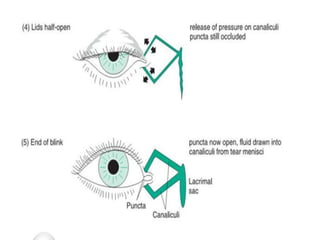


The lacrimal apparatus consists of the lacrimal gland, lacrimal drainage system, and associated structures that produce and drain tears from the eye. The lacrimal gland develops from surface ectoderm and is located above and lateral to the eye. Tears produced by the gland drain through puncta and canaliculi into the lacrimal sac, then through the nasolacrimal duct into the nose. The lacrimal sac is lodged in the lacrimal fossa of the medial orbital wall. It connects to the nasolacrimal duct, which courses posteriorly and laterally through bone to drain into the nasal cavity. Coordinated blinking and pressure differences aid























































































