Downloaded 39 times

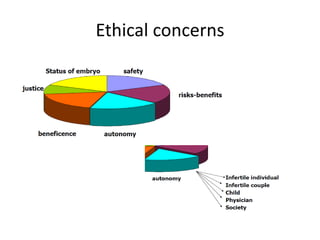

The document discusses ethics in assisted reproductive technologies (ART), outlining their development since the first successful IVF birth in 1978 and the subsequent moral and ethical dilemmas that arise, such as the definition of human life and patient autonomy. It addresses various concerns including societal implications, religious opposition, and the challenges of accessibility and discrimination in eligibility for IVF procedures. A case study highlights the ethical issues faced by a gay couple seeking IVF, ultimately being denied based on their sexual preference despite being financially able to proceed.































































![谷歌留痕技术 [ 𝙩𝙤𝙥 𝟮𝟯𝟯. 𝙘 𝙤𝙢 ]](https://cdn.slidesharecdn.com/ss_thumbnails/top233-260130174328-3833018c-thumbnail.jpg?width=640&height=640&fit=bounds)










