Esophageal varices and its management

This document discusses oesophageal varices, which are dilated and tortuous veins in the oesophageal wall that occur secondary to portal hypertension. It defines oesophageal varices and portal hypertension, and discusses the epidemiology, etiology, risk factors, clinical manifestations, diagnostic evaluations, medical and surgical management, nursing management, and complications of oesophageal varices. It also summarizes two research articles on using wireless capsule endoscopy to diagnose and grade varices, and using blood ammonia levels to predict the presence of varices and bleeding risk. The document concludes by emphasizing the importance for nurses to understand oesophageal varices to provide appropriate care and counseling to patients.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Esophageal varices and its management
Similar to Esophageal varices and its management (20)
More from Shweta Sharma
More from Shweta Sharma (20)
Recently uploaded
Recently uploaded (20)
Esophageal varices and its management
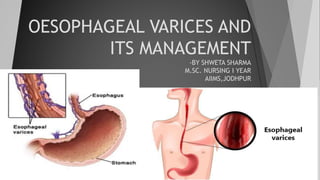
- 1. OESOPHAGEAL VARICES AND ITS MANAGEMENT -BY SHWETA SHARMA M.SC. NURSING I YEAR AIIMS,JODHPUR
- 2. DEFINITION Oesophageal varices are dilated and tortuous veins in the oesophageal wall, secondary to increased venous pressure in the splanchnic venous bed or in the superior vena cava. They are prone to rupture and often are the sources of massive haemorrhages from the upper gastro-intestinal tract and rectum.
- 3. PORTAL HYPERTENSION Normal pressure of portal vein is 5-8 mmHg. When it is >7-8mmHg, then called as portal hypertension. Symptoms and complications occur when the portal pressure is more than 12 mmHg.
- 4. EPIDEMIOLOGY •Present in 30% of patients with compensated cirrhosis and 60% of patients with decompensated cirrhosis at the time of diagnosis. •The first bleeding episode has a mortality rate of 10% to 30% depending on the severity of the liver disease and is one of the major causes of death in patients with cirrhosis. •Patients surviving the first episode of variceal bleeding are at very high risk for recurrent bleeding (approximately 70%) and death (30% to 50%).
- 5. ETIOLOGY Portal hypertension Abnormalities of the circulation in the splenic vein or superior vena cava Hepatic venothrombosis Severe liver scarring (cirrhosis) Blood clot (thrombosis) Parasitic infection- Schistosomiasis
- 7. RISK FACTORS High portal vein pressure Large varices Red marks on the varices Severe cirrhosis or liver failure Continued alcohol use
- 10. CLINICAL MANIFESTATIONS Hematemesis Melena General deterioration in mental or physical status Splenomegaly Ascites Sign and symptoms of shock (cool clammy skin, hypotension, tachycardia) may be present
- 11. FACTORS THAT CONTRIBUTE TO HEMORRHAGE Muscular exertion from lifting heavy objects Straining at stools Sneezing Coughing Vomiting Esophagitis Irritation of vessels by poorly chewed foods or irritating fluids Reflux of stomach contents (especially alcohol) Salicylates and any medication that erodes the oesophageal mucosa or interferes with cell replication
- 12. DIAGNOSTIC EVALUATION Endoscopy- To identify the cause and bleeding site.
- 13. Portal hypertension measurements Indirect measurement-
- 14. Direct measurement- During laparotomy, a needle may be introduced into the spleen; a manometer reading of more than 20 ml saline is abnormal. Insertion of a catheter into the portal vein or one of its branches. Endoscopic measurement of pressure within varices is used only in conjunction with endoscopic sclerotherapy.
- 15. Ultrasonography Computed tomography
- 22. Liver function tests- serum aminotransferase, bilirubin, alkaline phosphatase, serum proteins, etc.(increased) Splenoportography- To detect extensive collateral circulation in oesophageal vessels, which would indicate varices. Hepatic portography- X-ray visualization of the hepatic portal system made radiopaque by intravenous infusion of a suitable medium.
- 24. COMPLICATIONS •Hypovolemic or haemorrhagic shock •Hepatic encephalopathy- Due to increased nitrogen load from bleeding into the gastro-intestinal tract and an increased serum ammonia level. •Electrolyte imbalance •Metabolic and respiratory alkalosis
- 25. Oesophageal stricture after surgery or endoscopic therapy Infection (pneumonia, bloodstream infection, peritonitis) Rebleeding after treatment Kidney failure
- 26. MEDICAL MANAGEMENT Evaluate the extent of bleeding, monitor vital signs continuously if hematemesis and melena are present. Intravenous fluids to restore fluid volume. Parenteral nutrition Electrolytes to treat electrolyte imbalance. Volume expanders Blood transfusion Urinary catheterisation to monitor urine output. Gastric suction to keep the stomach as empty as possible and to prevent straining and vomiting.
- 27. Pharmacological therapy 1.Octreotide (sandostatin) – Synthetic analogue of the hormone somatostatin Effective in decreasing bleeding from oesophageal varices Lacks the vasoconstrictive effects of vasopressin Because of this safety and efficacy profile, it is considered the preferred treatment regimen for immediate control of variceal bleeding. Cause selective splanchnic vasoconstriction by inhibiting glucagon release and are used mainly in the management of active haemorrhage.
- 28. 2.Vasopressin (Pitressin)- It can be used as the initial mode of therapy in urgent situations because it produces constriction of the splanchnic arterial bed and decreases portal pressure. Contraindication – Coronary artery disease The combination of vasopressin with nitro-glycerine (administered by the IV, sublingual or transdermal route) has been effective in reducing or preventing the side effects caused by vasopressin alone. Side effects of vasopressin- myocardial and extremity ischemia as well as cardiac dysrhythmia.
- 29. 3.Beta-blocking agents- Propranolol or nadolol that decrease portal pressure. Used both to prevent a first bleeding episode in patients with known varices and to prevent rebleeding. They should not be used in acute variceal haemorrhage, but they are effective prophylaxis against such an episode. 4.Nitrates such as isosorbide (Isordil)- •Lower portal pressure by venodilation and decreased cardiac output and may be used in combination with beta-blockers.
- 33. Endoscopic variceal ligation (oesophageal banding therapy)-
- 35. Trans jugular intrahepatic portosystemic shunt (TIPS)
- 38. SURGICAL MANAGEMENT Surgical bypass procedure- Distal splenorenal shunt
- 40. Devascularization and transection (Sugiura procedure)-
- 41. NURSING MANAGEMENT Nursing assessment- •Monitor the patient’s physical condition and evaluate emotional responses and cognitive status. •Monitor and record the vital signs. •Assess the patient’s nutritional and neurologic status. •Provide oral hygiene and moist sponges to lips. •Provide a quiet environment and calm reassurance may help to relieve the patient’s anxiety and reduce agitation.
- 42. NURSING DIAGNOSIS Fluid volume deficit related to active bleeding as evidenced by decreased urine output (less than 30mL/hr). Ineffective tissue perfusion related to hypovolemia as evidenced by abnormal arterial blood gases. Anxiety related to change in health status as evidenced by irritability and nervousness due to bleeding.
- 43. PREVENTION Don't drink alcohol Eat a healthy diet. Maintain a healthy weight. Use chemicals sparingly and carefully. Reduce your risk of hepatitis.
- 44. RESEARCH ARTICLES 1.Use of Wireless Capsule Endoscopy for the Diagnosis and Grading of Esophageal Varices in Patients with Portal Hypertension: A Systematic Review and Meta-analysis A systematic review and structured meta-analysis was performed of all eligible studies to evaluate the efficacy of wireless capsule endoscopy for screening and diagnosis of esophageal varices among patients with portal hypertension. Seventeen studies from 2005 to 2015 were included in this meta-analysis. The diagnostic accuracy of wireless capsule endoscopy in the diagnosis of esophageal varices was 90%. The diagnostic accuracy of wireless capsule endoscopy for the grading of medium to large varices was 92%. The use of capsule demonstrated only mild adverse events. The study concluded that wireless esophageal capsule endoscopy is well tolerated and safe in patients with liver cirrhosis and suspicion of portal hypertension.
- 45. 2.Evaluation of the blood ammonia level as a non-invasive predictor for the presence of oesophageal varices and the risk of bleeding. A cross -sectional study was performed on a total of 359 patients with cirrhosis. The aim of this study was to evaluate the blood ammonia level as a predictor of the presence of esophageal varices and of a high risk of bleeding. Abdominal ultrasonography, calculation of the Child-Pugh score, and measurement of blood ammonia were performed for each patient. The blood ammonia level was significantly higher in patients with esophageal varices than in those without it, and in patients with a high risk of variceal bleeding than in those with a low risk. The study concluded that blood ammonia level may be clinically useful as it correlates with and is an independent predictor for both the endoscopic risk signs and risk factors of bleeding, and therefore, it could be used in patients with cirrhosis to decrease the number of screening endoscopies they are subjected to.
- 47. CONCLUSION As discussed throughout the presentation, learning about oesophageal varices and its management will help nurses to care for patients of oesophageal varices. Nurses can do assessment of patients with oesophageal varices, observe the sign and symptoms, provide the necessary nursing care, prevent complications and support the patient psychologically. Nurses can also counsel the patients and their family for various options available in treatment for oesophageal varices.
- 48. REFERENCES 1.Janice L. Hinkle, Kerry H. Cheever. Brunner and Suddarth’s Textbook of Medical Surgical Nursing. 2015. New Delhi. Wolters Kluwer.13th Edition. Volume 2. Pg. no. 1349-1354. 2.Lewis. Medical Surgical Nursing Assessment and Management of clinical problems.2015. New Delhi. Elsevier. 2nd Edition. Volume II. Pg. no.998, 1068. 3.Mayo Clinic. Oesophageal varices. Available from https://www.mayoclinic.org/diseases- conditions/esophageal-varices/symptoms-causes/syc- 20351538#:~:targetText=Esophageal%20varices%20are%20abnormal%2C%20enlarged,scar%2 0tissue%20in%20the%20liver. [cited 8 nov 2019] 4.PubMed. Use of Wireless Capsule Endoscopy for the Diagnosis and Grading of Esophageal Varices in Patients With Portal Hypertension: A Systematic Review and Meta-Analysis. Available from https://www.ncbi.nlm.nih.gov/pubmed/27548729 [cited 8 nov 2019] 5.PubMed. Evaluation of the blood ammonia level as a non-invasive predictor for the presence of esophageal varices and the risk of bleeding. Available from https://www.ncbi.nlm.nih.gov/pubmed/30465524 [cited 8 nov2019]