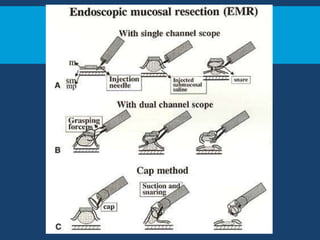
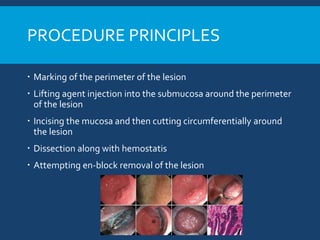
Endoscopic submucosal dissection (ESD) is an endoscopic procedure that allows for en bloc resection of gastrointestinal lesions. Key aspects of ESD include injecting a lifting agent into the submucosa to elevate the lesion prior to marking the margins and performing a circumferential mucosal incision and submucosal dissection. ESD provides improved resection rates compared to endoscopic mucosal resection and allows for specimen retrieval intact for accurate histological assessment. While complications such as bleeding and perforation can occur, most are often managed endoscopically without need for surgery. ESD has become a standard treatment for early gastrointestinal cancers and pre-cancers when criteria for curative resection are met.