Downloaded 312 times







































![Completion surgery
Demonstrated to be safe and return oncological outcome to that of primary TME surgery for
matched tumour groups.
In a series of 105 patients undergoing TEM for T1 rectal cancer the local recurrence rate was
6% for low risk T1 tumours with R0 resection whereas rate in the high risk group was 39%.
10 year follow up the cancer free survival was 93% in the reoperation
group and 89% in the TEMS alone group. This effect is seen in series where local excision
(other than TEMS) is used where immediate reoperation in high risk groups reduced
recurrence from 50% (non-operated) to 7.7% (operated). A recent case matched study no
difference was found in outcome between patients with rectal cancer undergoing completion
TME after TEMS (n ¼ 25) compared to those undergoing primary TME (n ¼ 25), with similar
pre and peri-operative parameters.
Recurrence was 0% in the completion group and 8% (p ¼ 0.49) in the primary group. Follow up
was short however, with a median of only 25 months (range of 3–126) but no difference in rates
of distant metastases was observed (4% v 12%, p0.61) [66].](https://image.slidesharecdn.com/tem-new-180411053820/75/Trans-anal-Endoscopic-Microsurgery-TEM-50-2048.jpg)

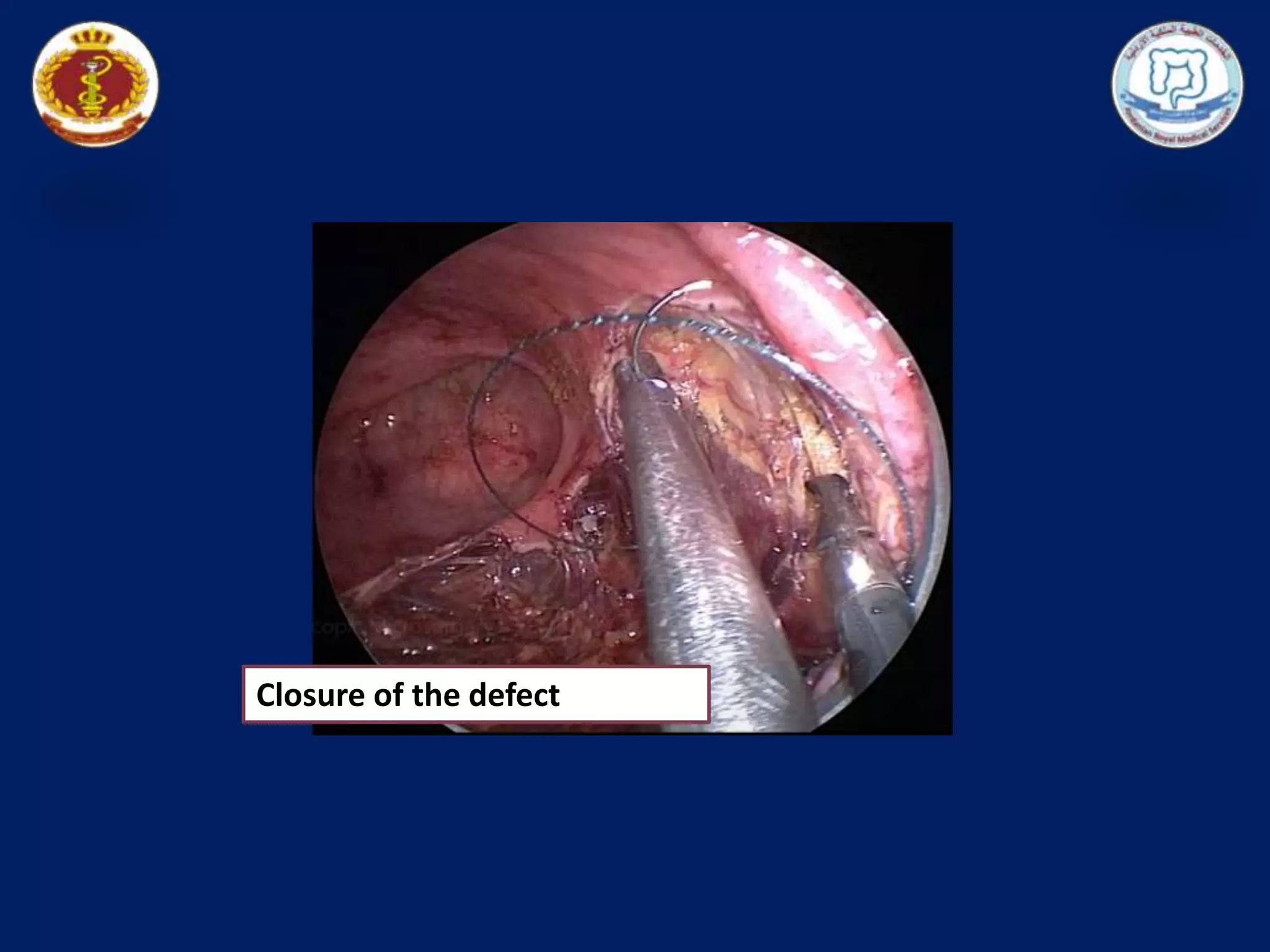
Dr. Khaled Mestareehy discusses transanal endoscopic microsurgery (TEM) for managing rectal tumors, including case presentations of two male patients treated with TEM. TEM is emphasized as a minimally invasive technique that preserves sphincter function while eradicating malignancies without the complications of major transabdominal surgery. Guidelines for patient selection, management, and outcomes for early rectal cancers and the technique's notable safety profile are outlined.












































































