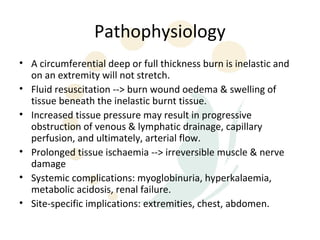
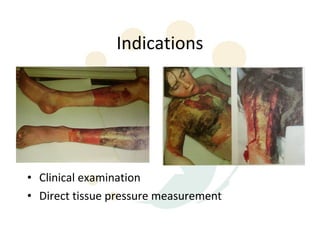
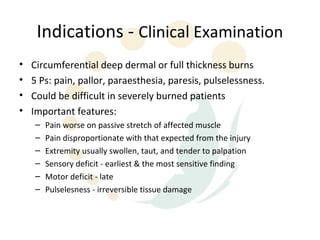
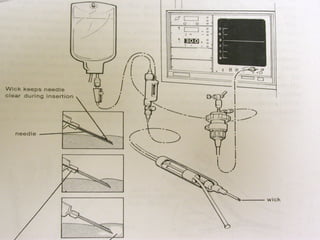
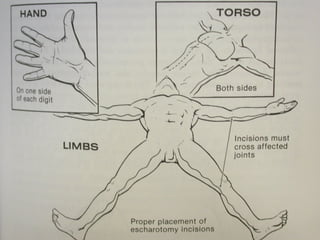
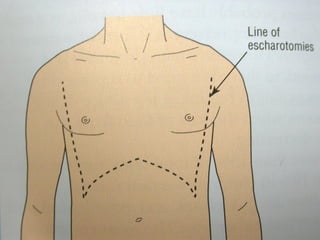
Escharotomy is used to decompress constrictive effects caused by deep circumferential burns. The eschar forms a tight inelastic layer over swollen tissue, obstructing blood flow. Indications for escharotomy include circumferential deep dermal or full thickness burns with signs of vascular compromise like pain, pallor, numbness. Tissue pressure monitoring can objectively measure compartment pressures, with surgical decompression recommended over 30-40 mmHg. Proper escharotomy incisions must fully traverse the eschar depth and length to relieve constriction while avoiding major structures. Timely escharotomy preserves tissue and function by relieving ischemia.