Downloaded 645 times
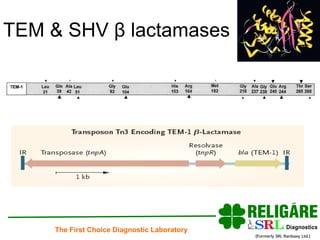
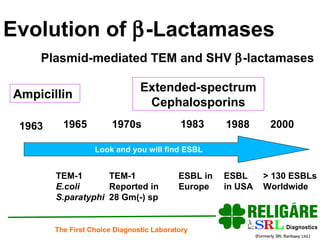
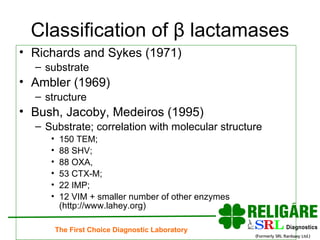
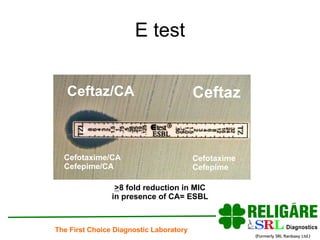

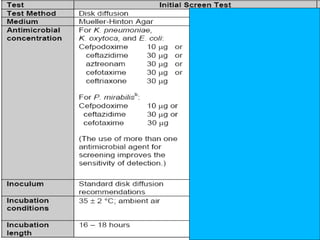
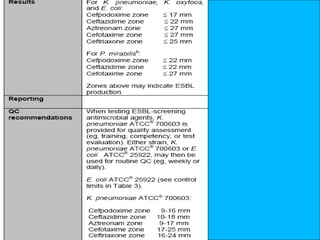
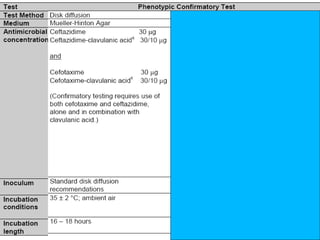
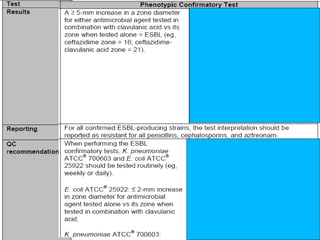

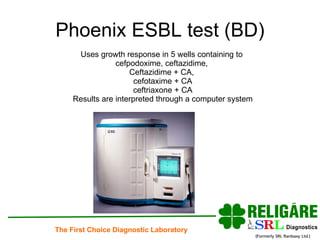

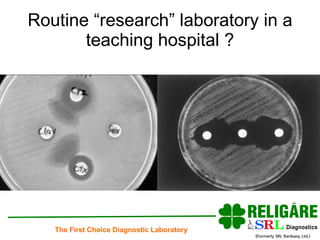
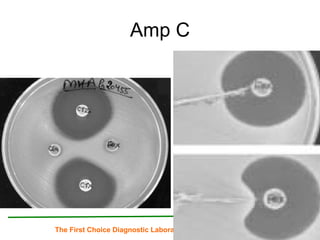





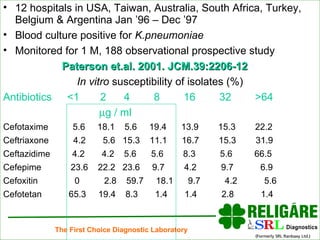
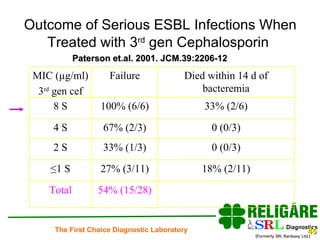

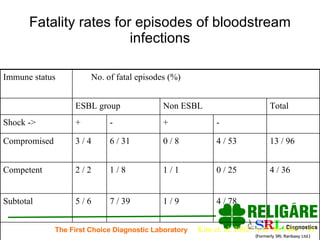
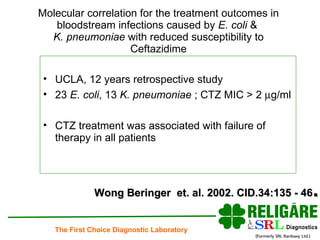
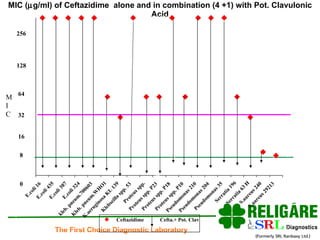
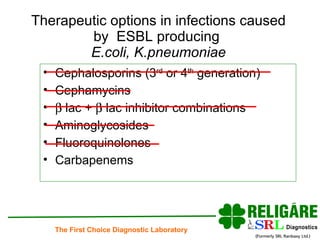
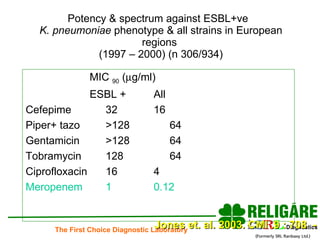
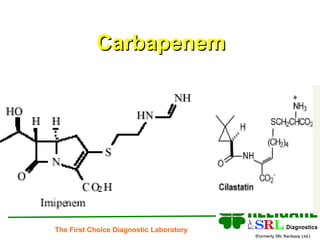
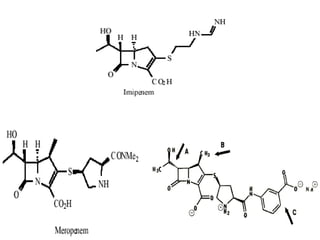
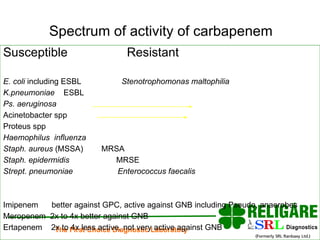


The document discusses extended spectrum beta-lactamases (ESBL), emphasizing their evolution, classification, detection methods, and clinical implications in treating infections caused by resistant bacteria. It highlights the importance of laboratory detection and appropriate antibiotic use, particularly avoiding third and fourth-generation cephalosporins for ESBL-producing organisms. Additionally, it outlines various therapeutic options and the significance of effective infection control measures in healthcare settings.



















































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)



![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)