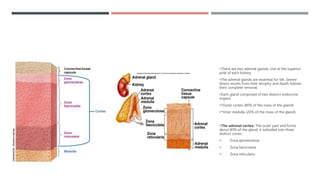
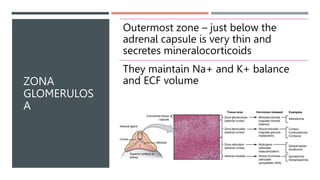
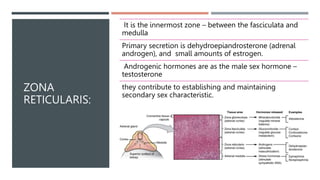
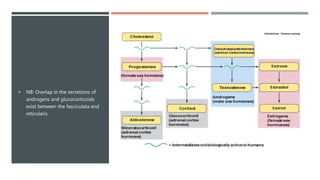
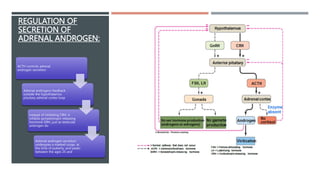
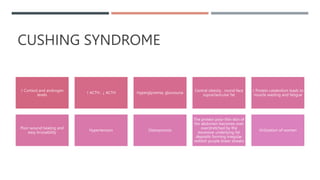
The adrenal glands produce important hormones including cortisol, aldosterone, and adrenal androgens. Each gland is composed of an outer cortex and inner medulla. The cortex is divided into three zones producing different hormones. The zona glomerulosa produces mineralocorticoids like aldosterone. The zona fasciculata produces glucocorticoids like cortisol. The zona reticularis produces small amounts of sex hormones. Disorders of the adrenal glands can cause too little or too much production of these hormones, leading to diseases like Addison's disease or Cushing's syndrome with their associated signs and symptoms.