Download to read offline
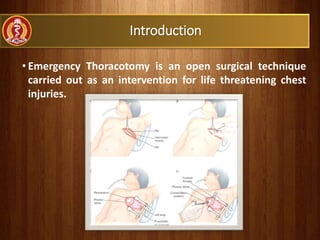
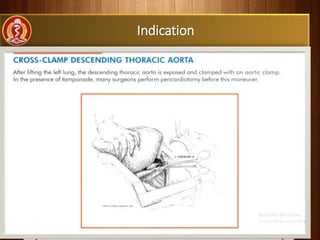
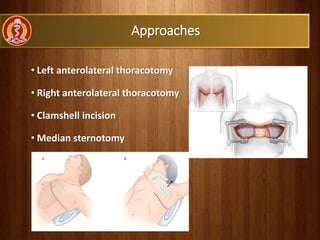


Emergency thoracotomy is a critical surgical procedure performed for life-threatening chest injuries, addressing conditions such as pericardial tamponade and massive hemorrhage. There are specific types, indications, and contraindications, with various surgical approaches and potential complications. Proper management following surgery, including chest drain monitoring, is vital for recovery.







































![Chest_trauma types and management[1].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/malamulochesttrauma1-241126062258-4b388e87-thumbnail.jpg?width=640&height=640&fit=bounds)
![management of Chest_trauma for nursing [1].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/malamulochesttrauma1-241127110255-71befbaa-thumbnail.jpg?width=640&height=640&fit=bounds)
































