Downloaded 37 times
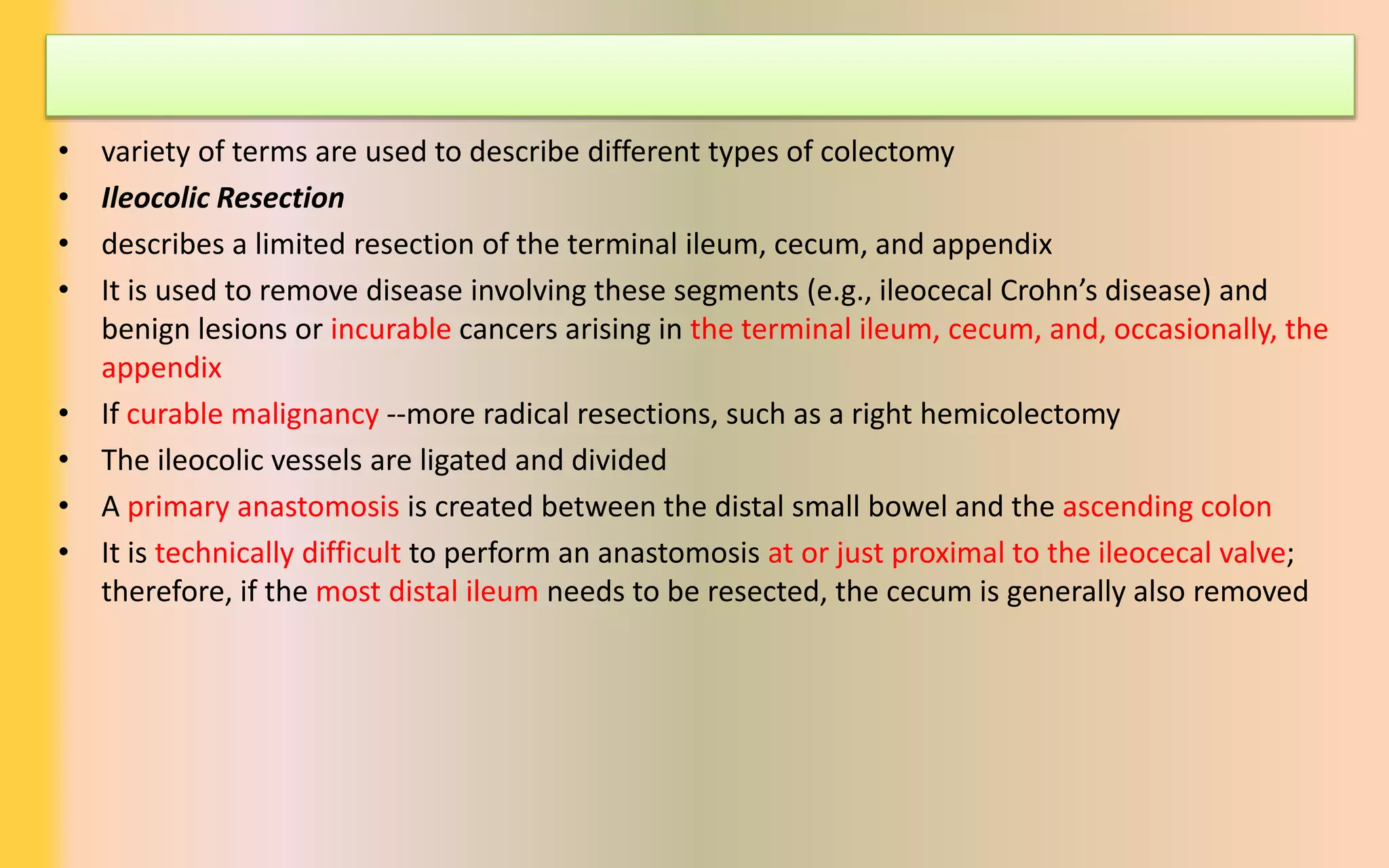

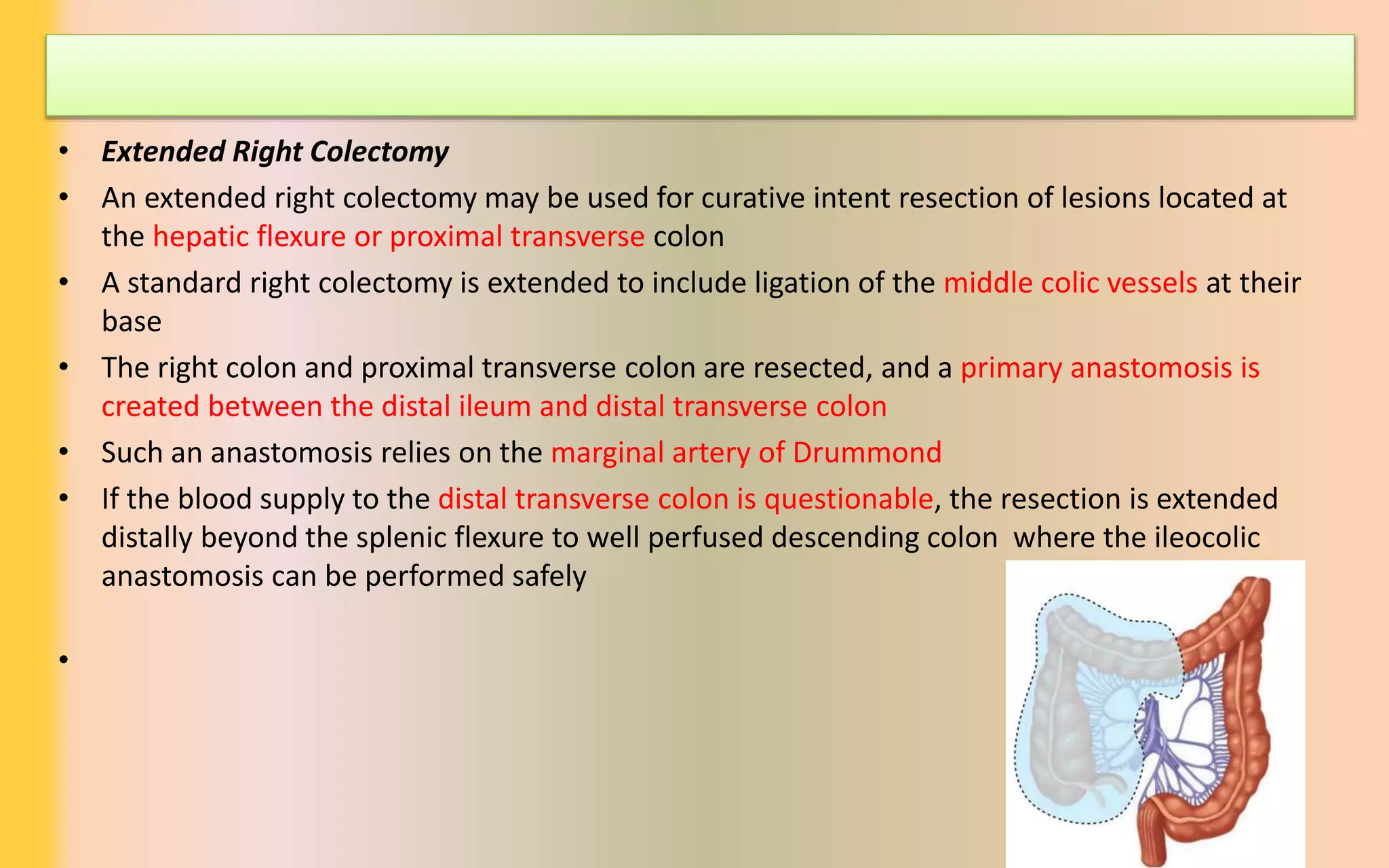
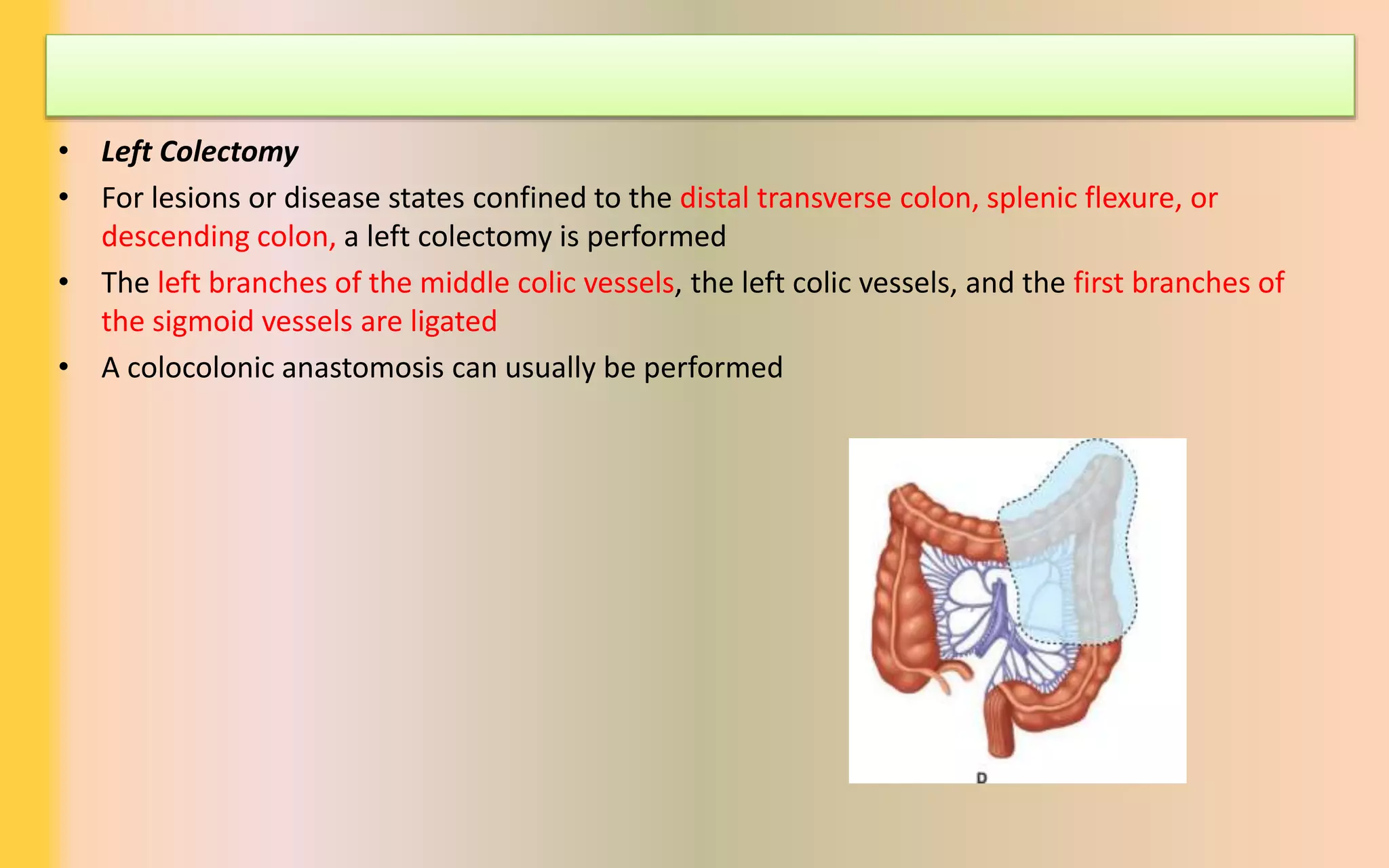
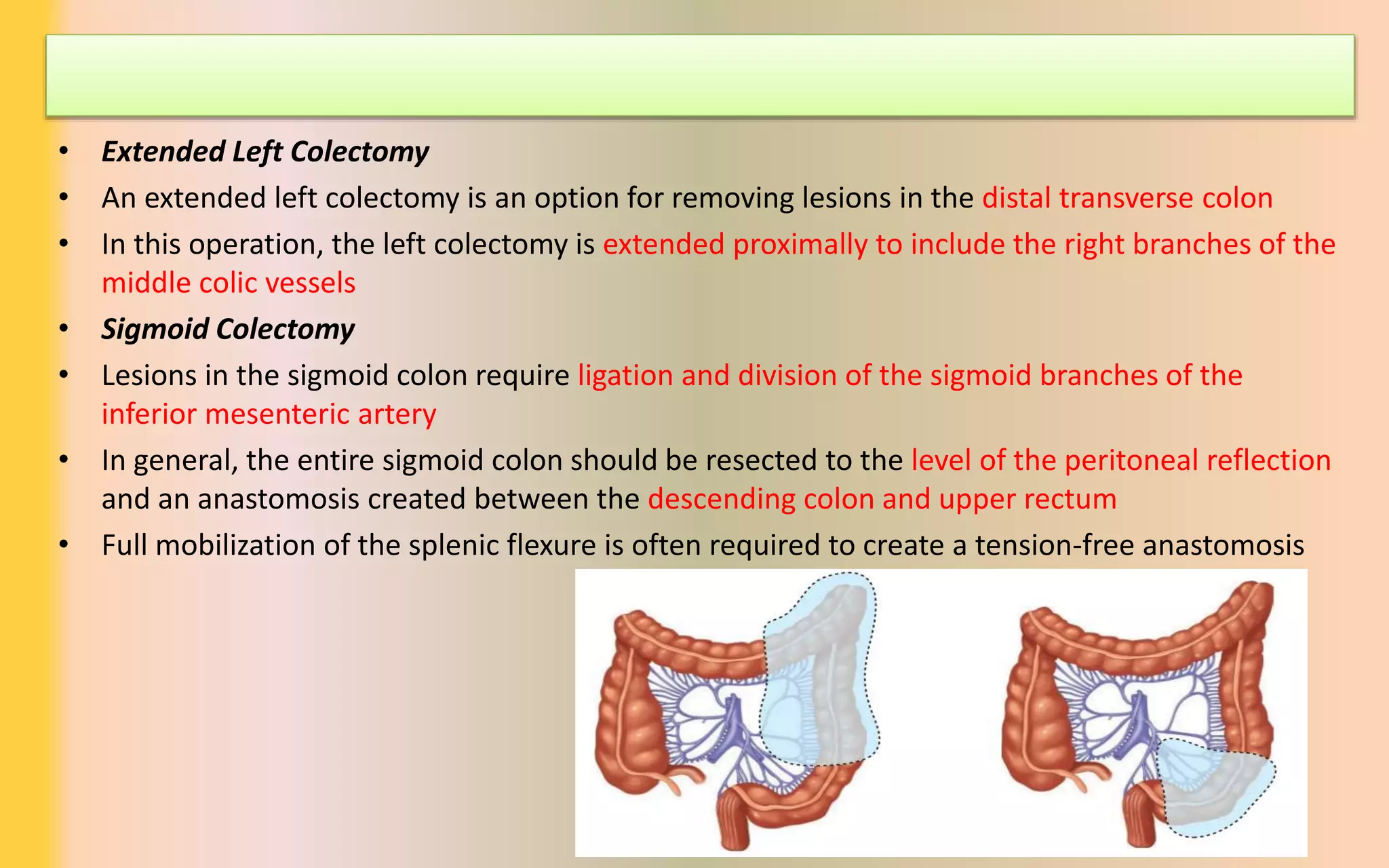


The document discusses various types of colectomy procedures, including ileocolic, right, transverse, left, sigmoid, total, subtotal colectomy, and proctocolectomy, outlining their indications and surgical techniques. Each colectomy type addresses specific lesions or diseases, detailing vessel ligation, resection areas, and anastomosis creation. It highlights the technical difficulties and considerations for ensuring adequate blood supply during surgeries.




















































































