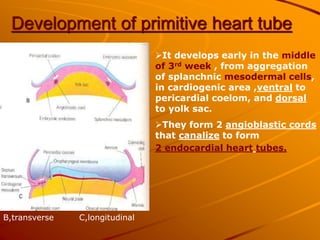
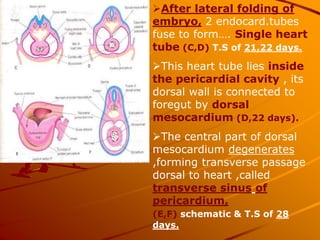
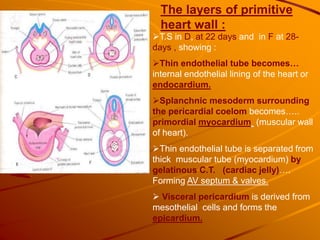
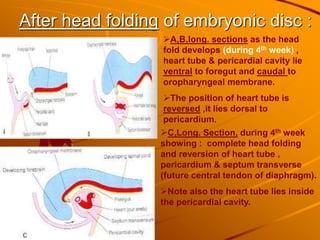
1) The primitive heart tube develops from splanchnic mesoderm and forms endocardial heart tubes that fuse to form a single heart tube.
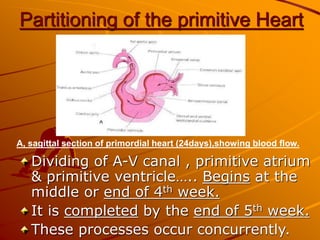
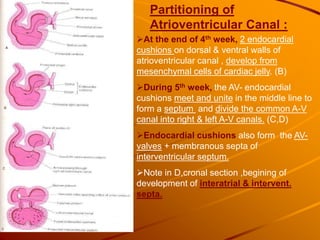
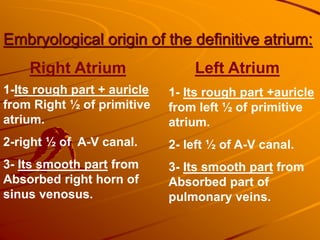
2) Partitioning of the heart begins around the 4th week as septa form to divide the atria and ventricles. The atrioventricular canal is divided by endocardial cushions fusing in the middle.
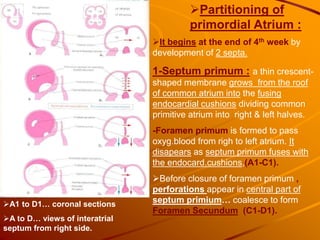
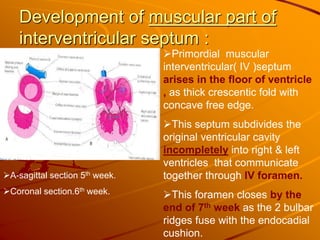
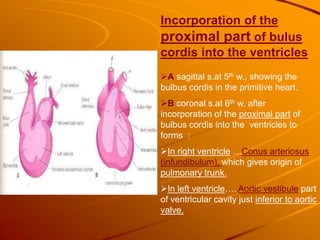
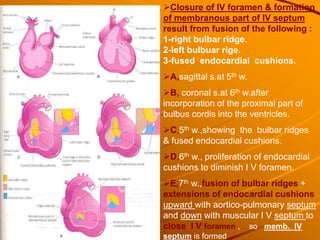
3) By the 5th week, the interventricular foramen closes as bulbar ridges fuse with endocardial cushions, completing partitioning of the heart into four chambers.


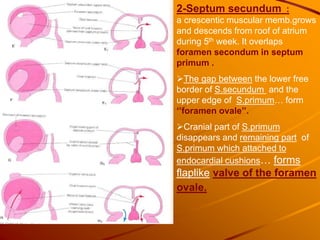





![Embryology [heart.].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/embryologyheart-230508191331-cc41d237-thumbnail.jpg?width=640&height=640&fit=bounds)



























































