
Downloaded 204 times


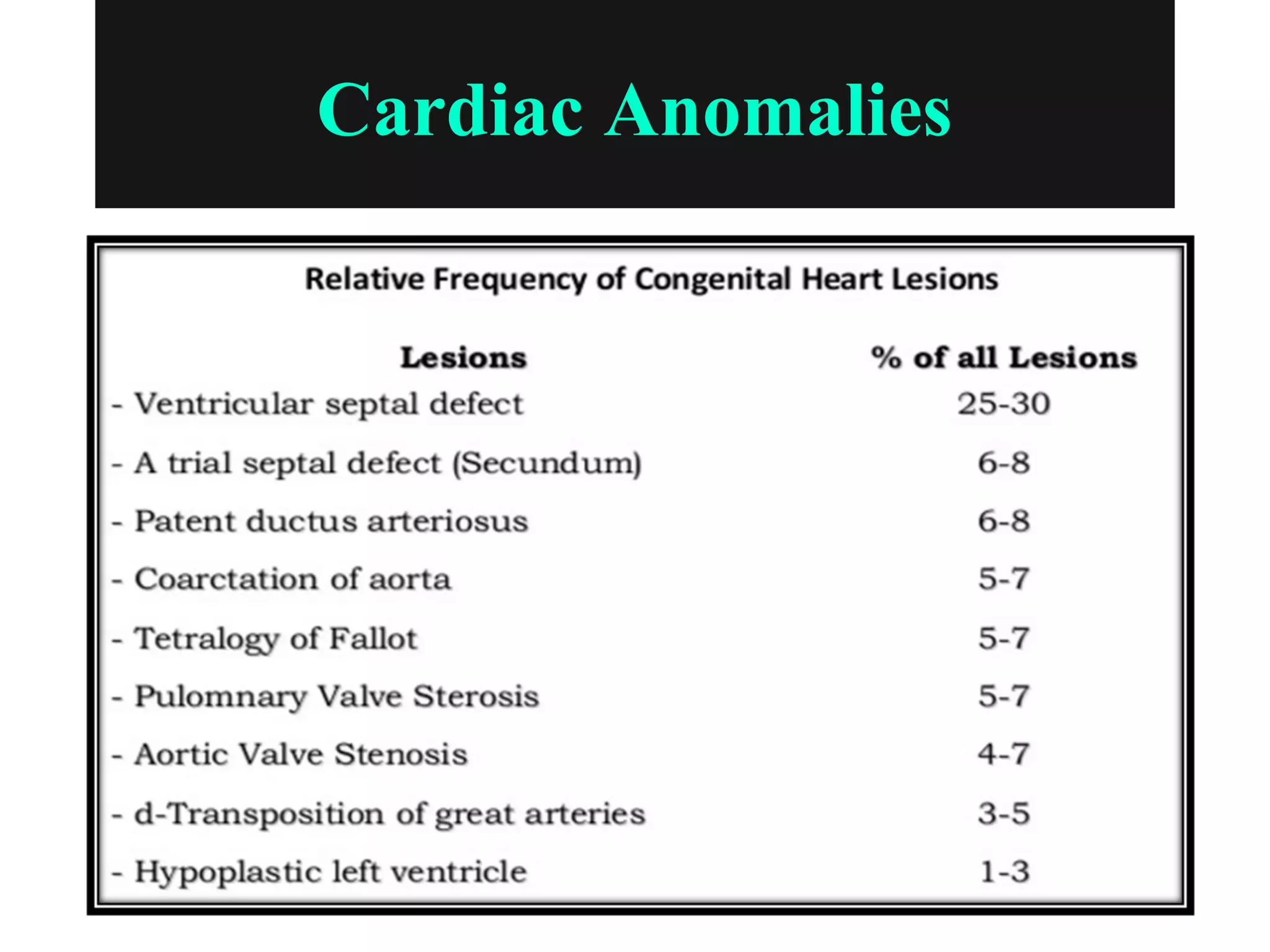
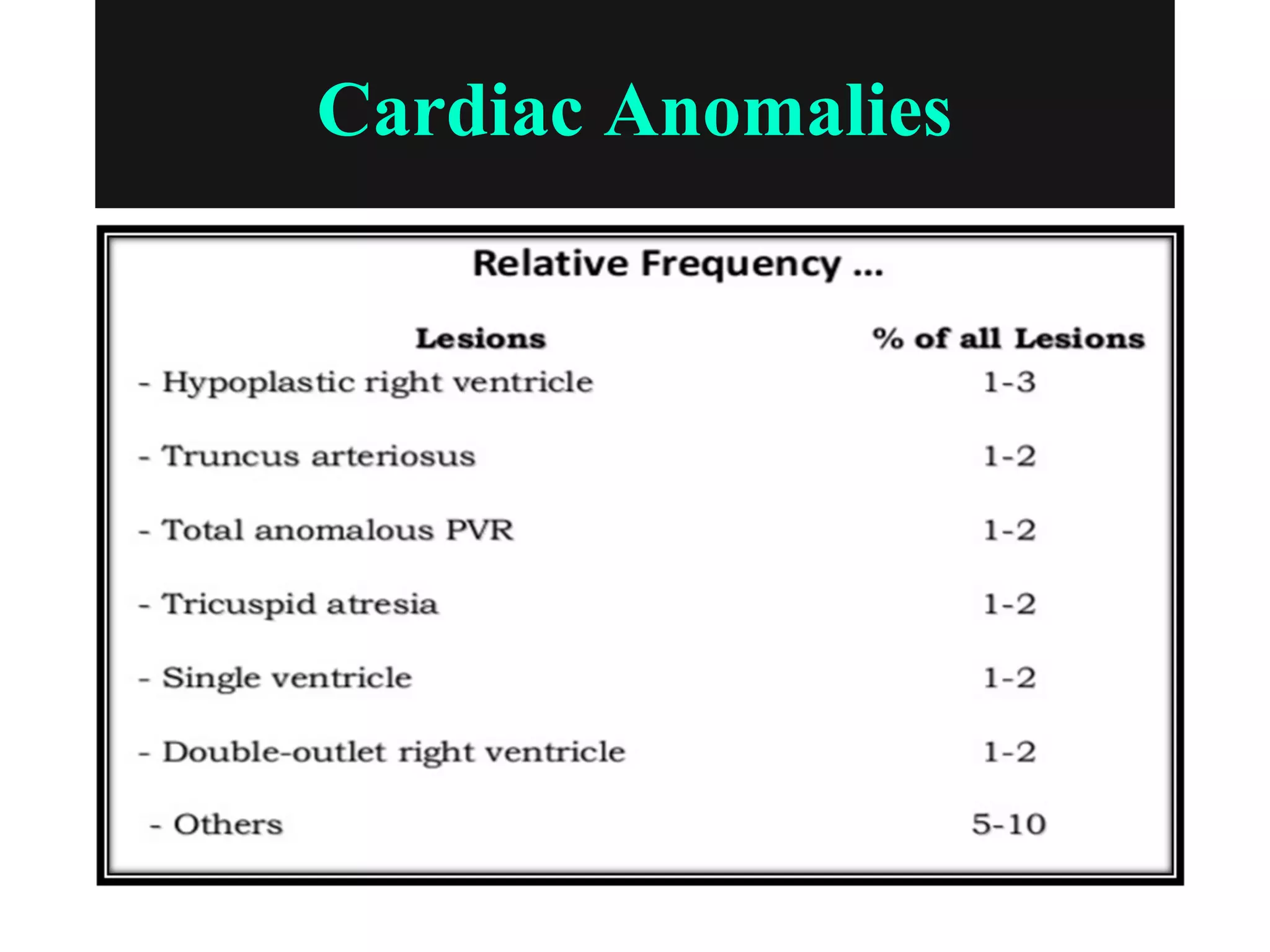



















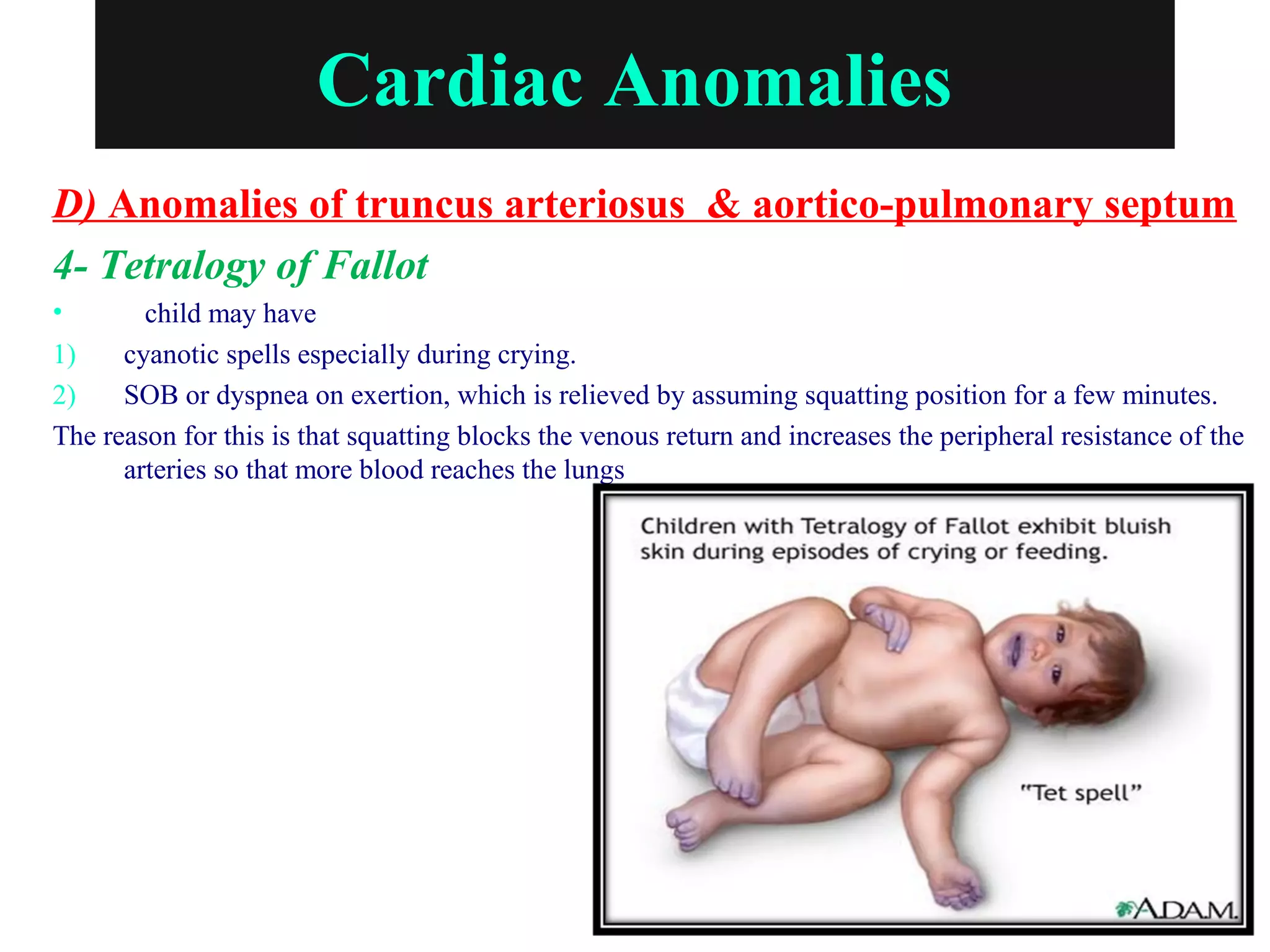


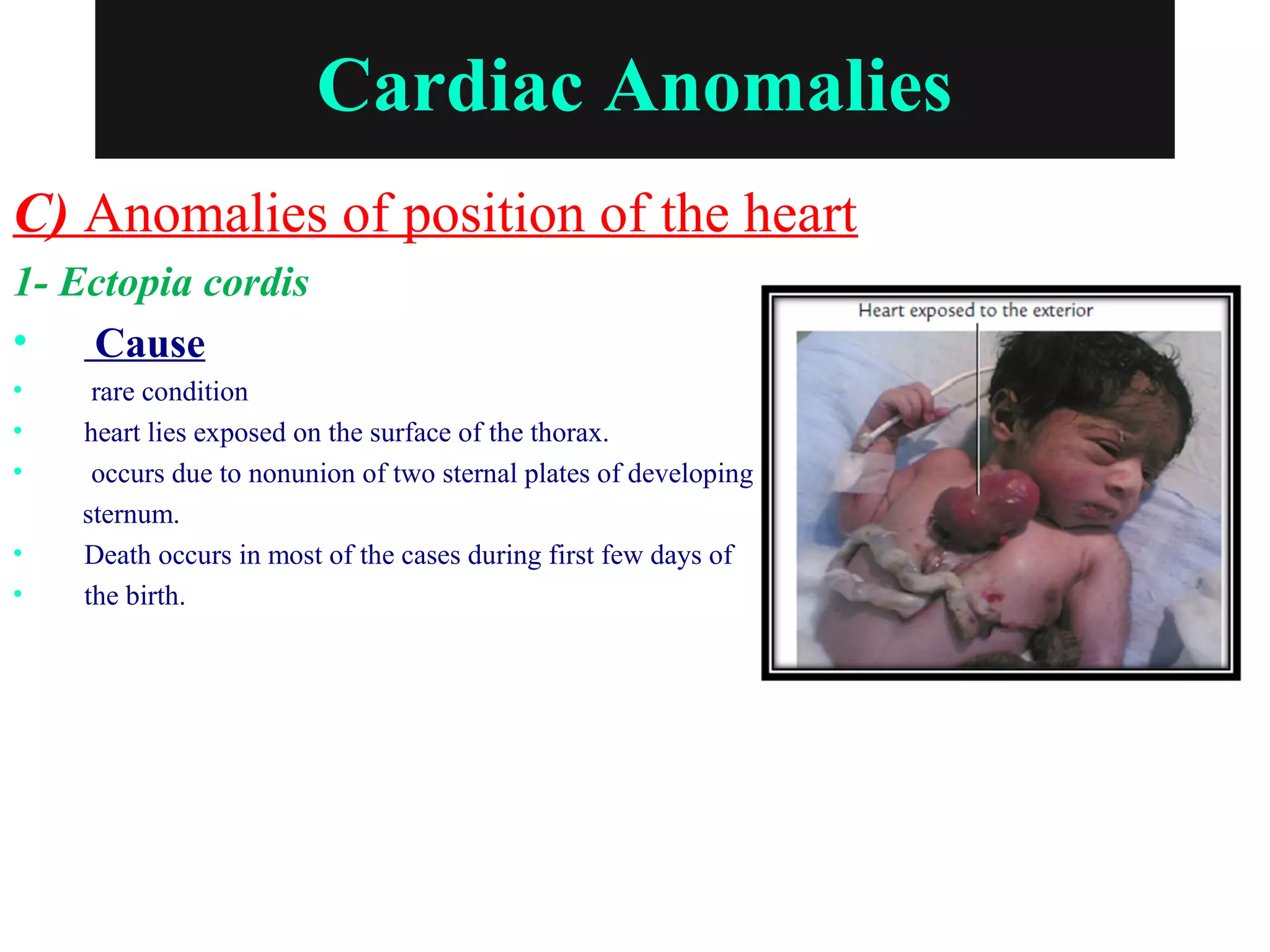




This document outlines the embryological basis of congenital heart diseases, detailing their incidence, etiological factors, and various cardiac anomalies such as atrial and ventricular septal defects, atrioventricular canal defects, and traduced anomalies related to truncus arteriosus. Genetic factors, environmental influences, and maternal health conditions during pregnancy contribute to the development of these congenital defects. The document also emphasizes distinguishing between cyanotic and acyanotic congenital heart diseases, providing clinical implications for diagnosis and management.























































































