Downloaded 15 times















































Congenital heart defects (CHD) are anatomical malformations of the heart present at birth, affecting about 0.8% of live births and divided into noncyanotic and cyanotic types. CHDs are the leading cause of birth defect-related death, with common forms including ventricular septal defect (VSD) and atrial septal defect (ASD), among others. Diagnosis often requires specific clinical findings and treatments may involve surgical interventions, especially for significant defects or those causing symptoms.
Presentation title. Introduction to Siambi Philip's work on congenital heart defects.
CHD prevalence (0.8% of births), types: noncyanotic and cyanotic; leading cause of birth defect death.
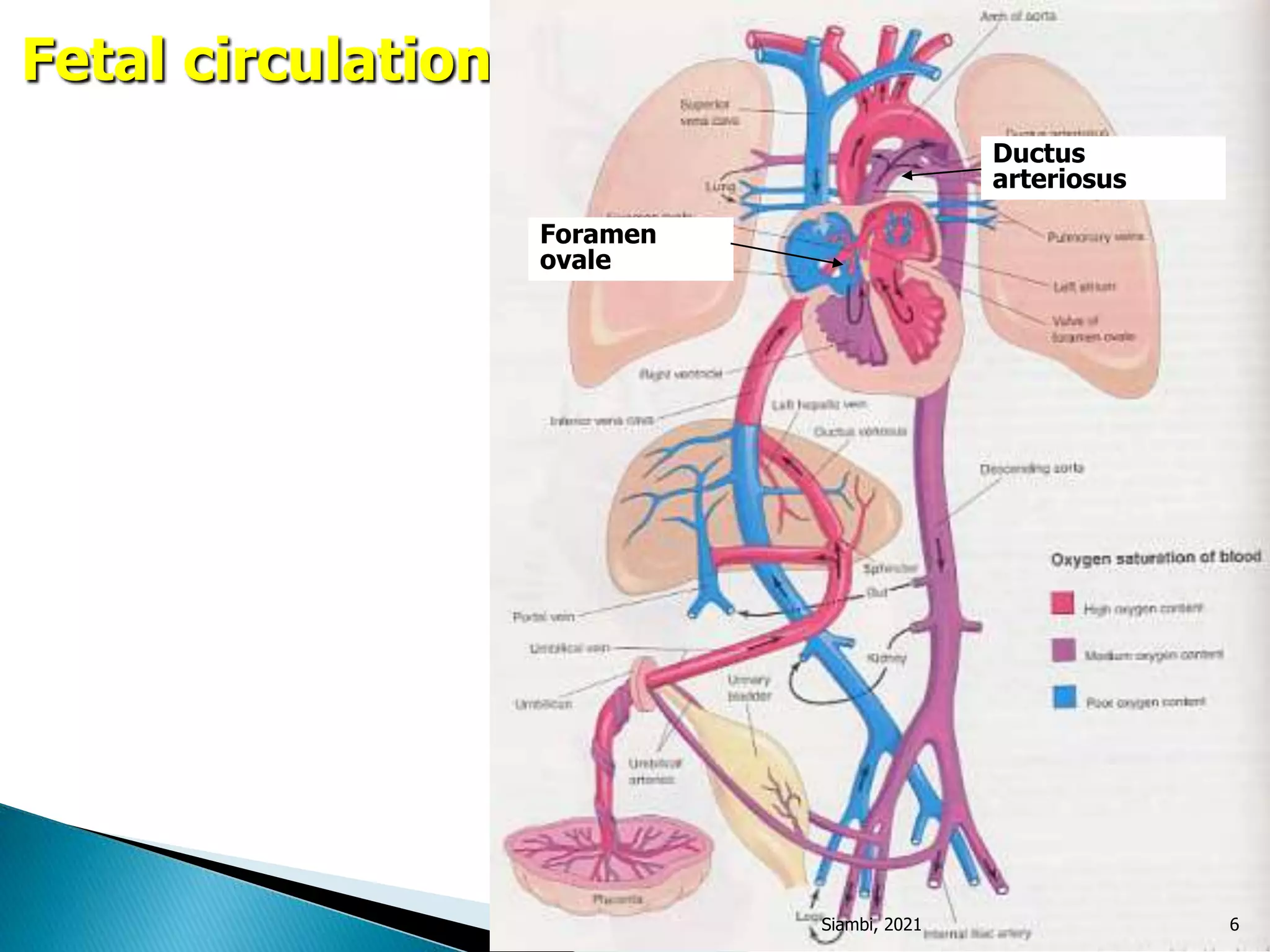
Fetal circulation's unique pathways (foramen ovale, ductus arteriosus) and implications post-birth.
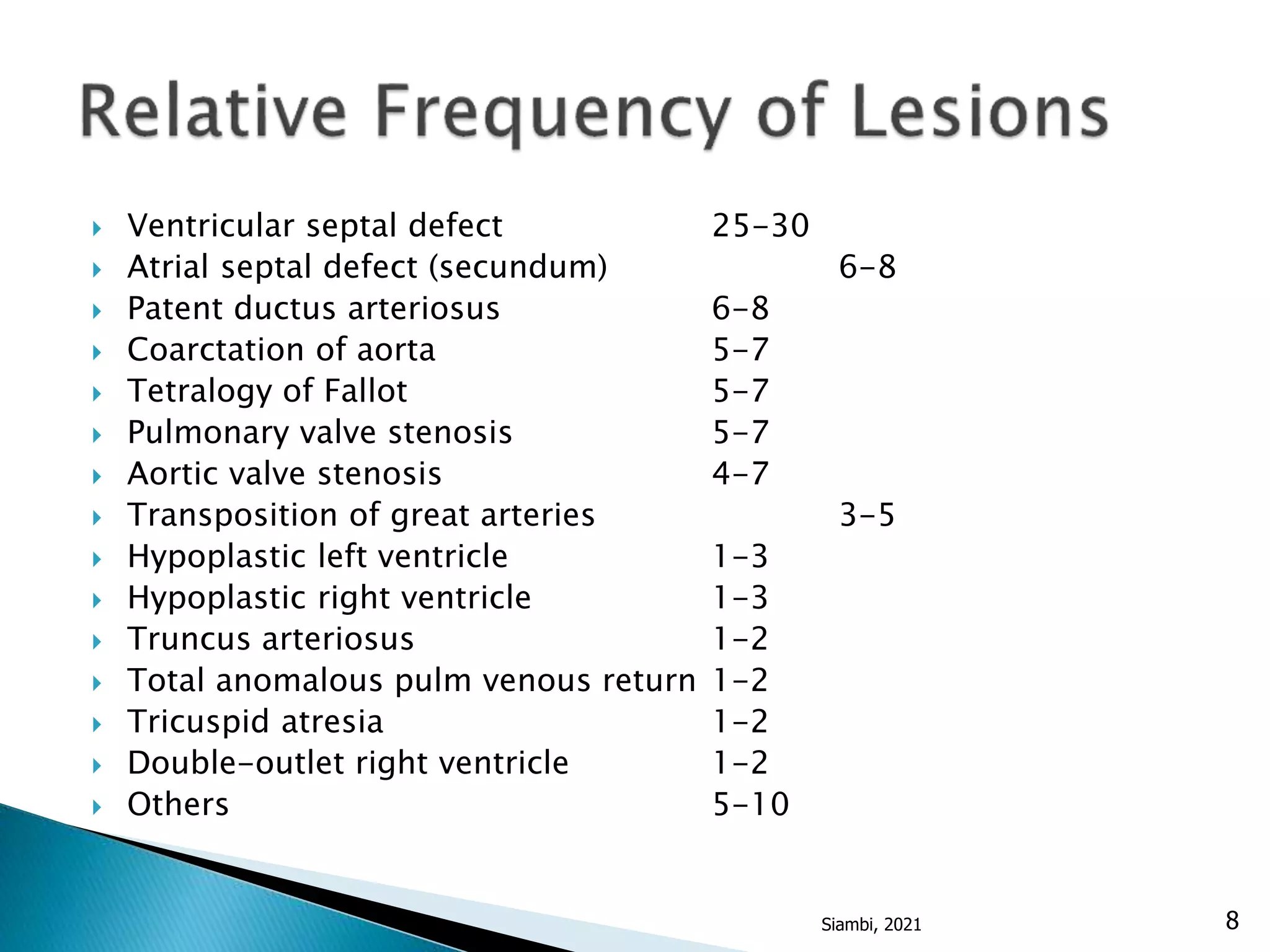
Common defects: VSD (25-30%), ASD (6-8%), PDA (6-8%); various obstructions detailed.
ASD types: secundum, primum, sinus venosus; treatment guidelines and timing for closure.
Most common CHD; symptoms, unexpected closure rates, treatment criteria for varying VSD sizes.
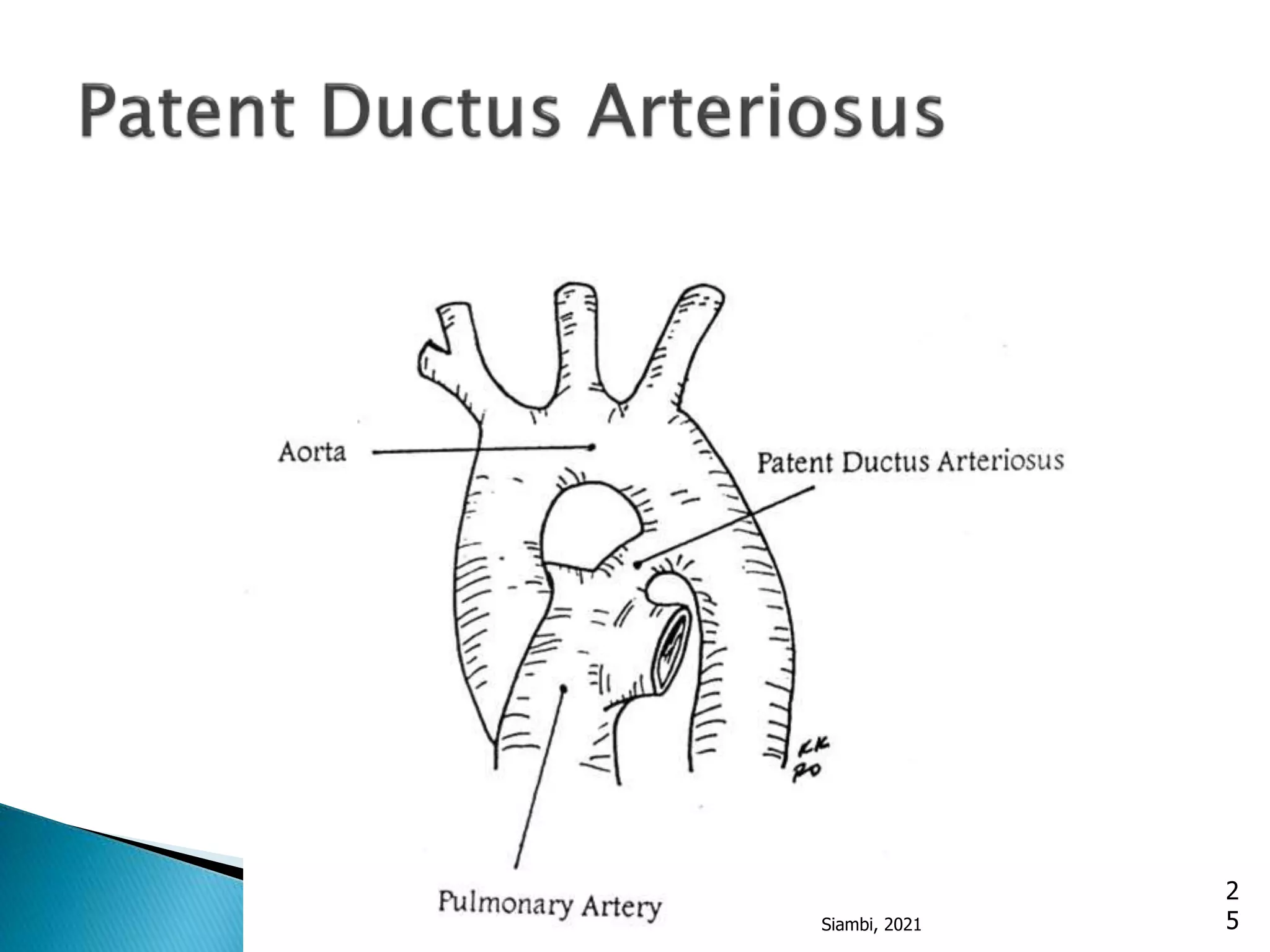
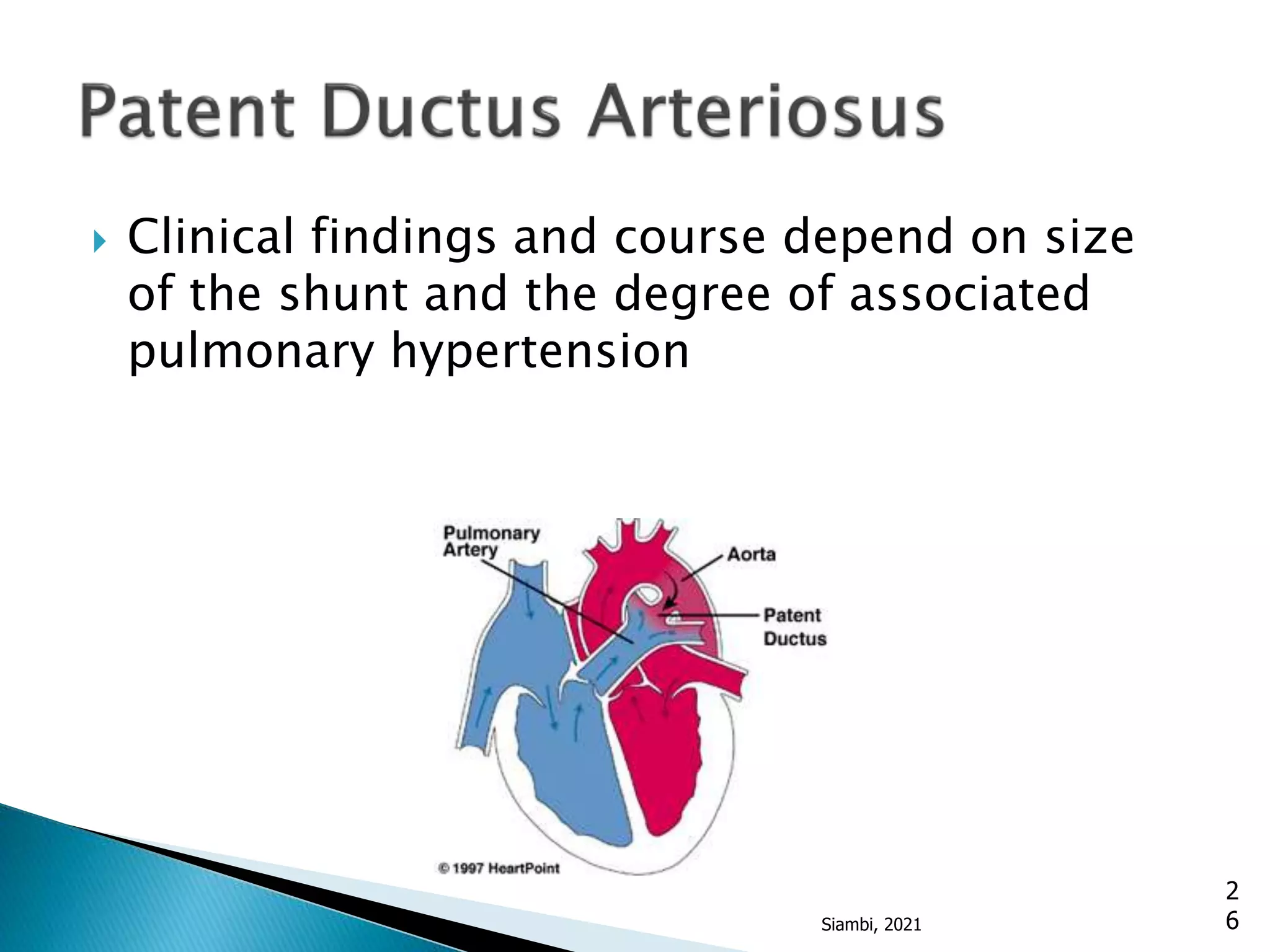
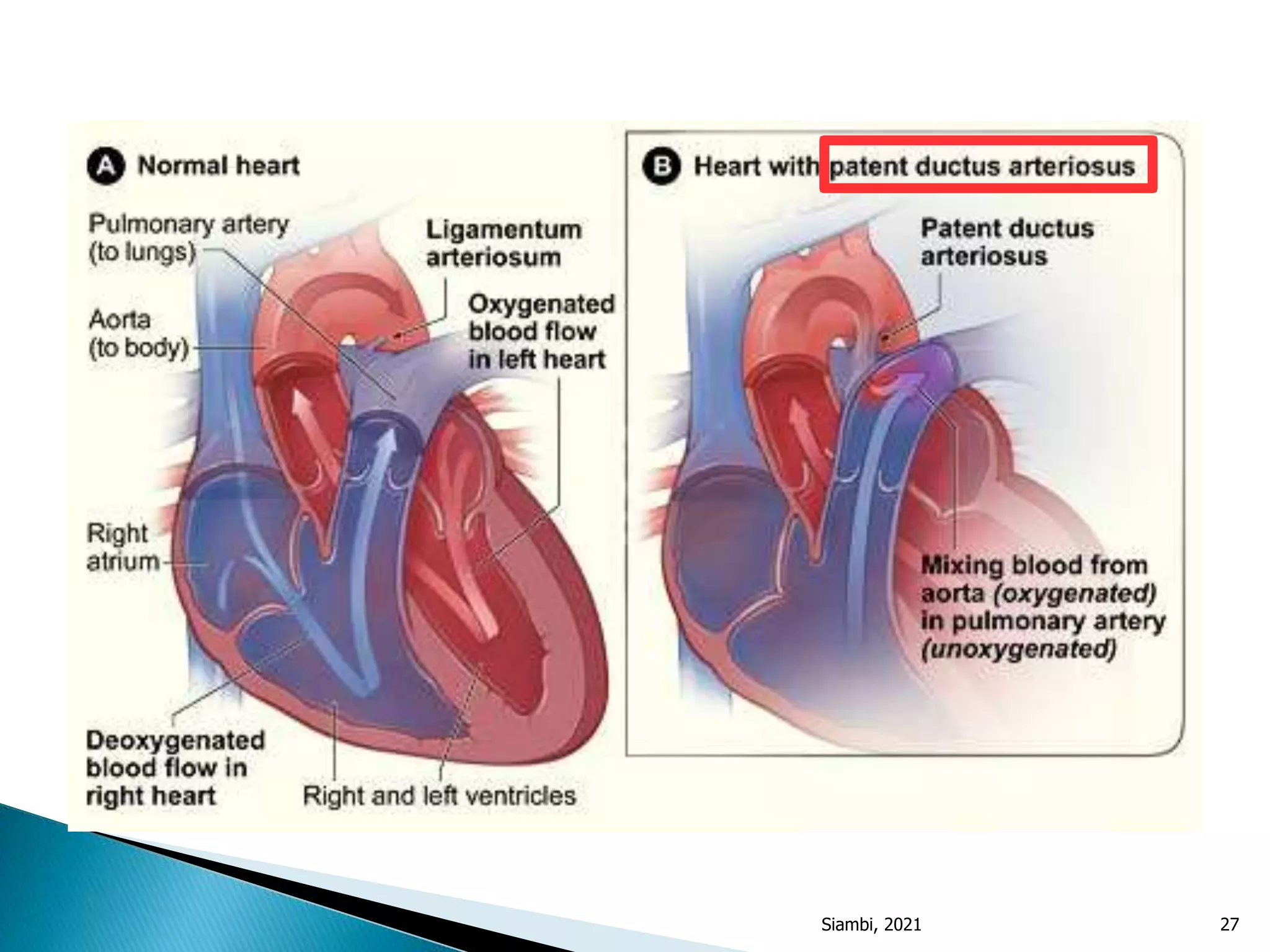
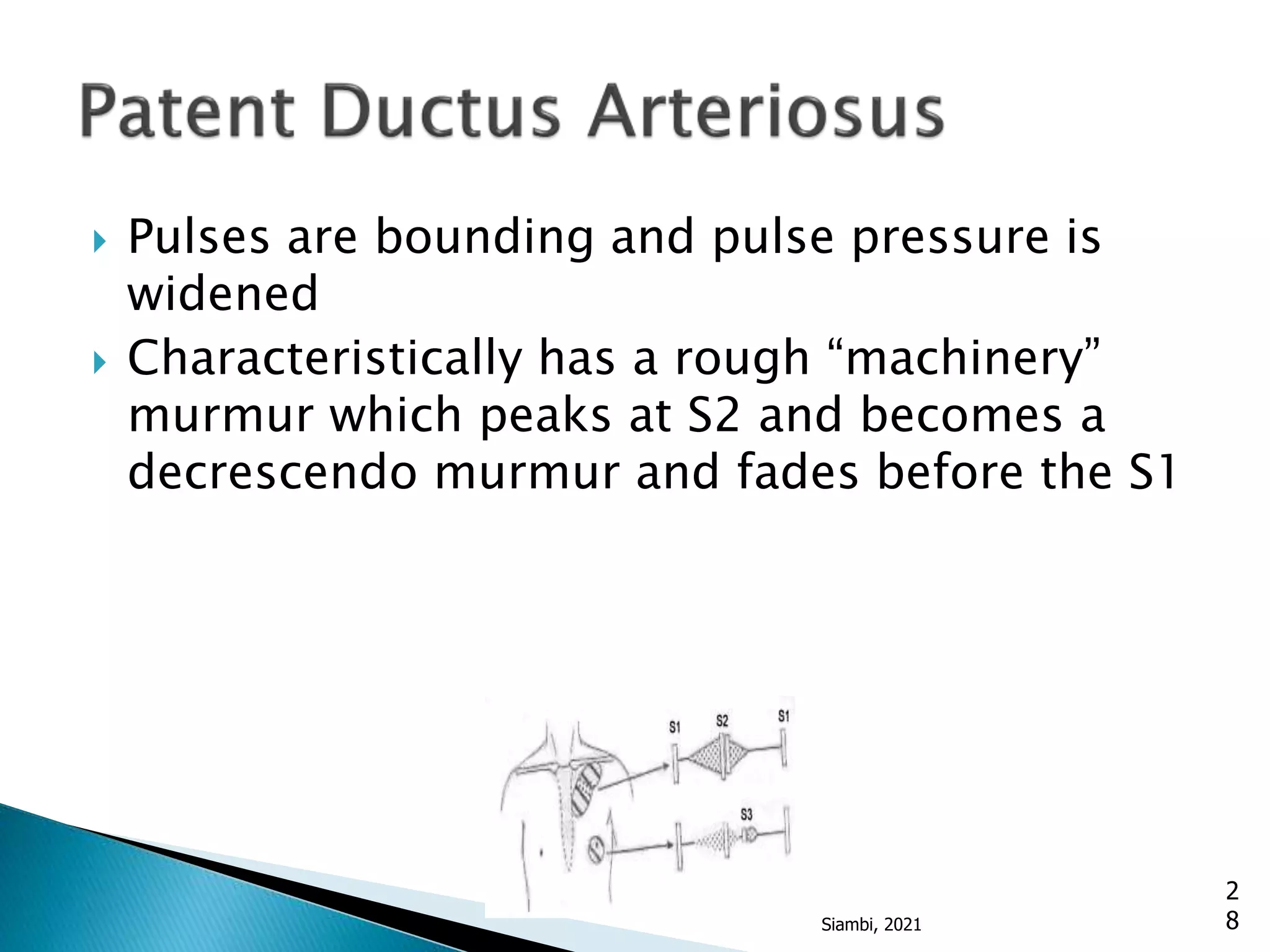
PDA accounted for 10% CHD; closure usually spontaneous; treatment includes surgical options.
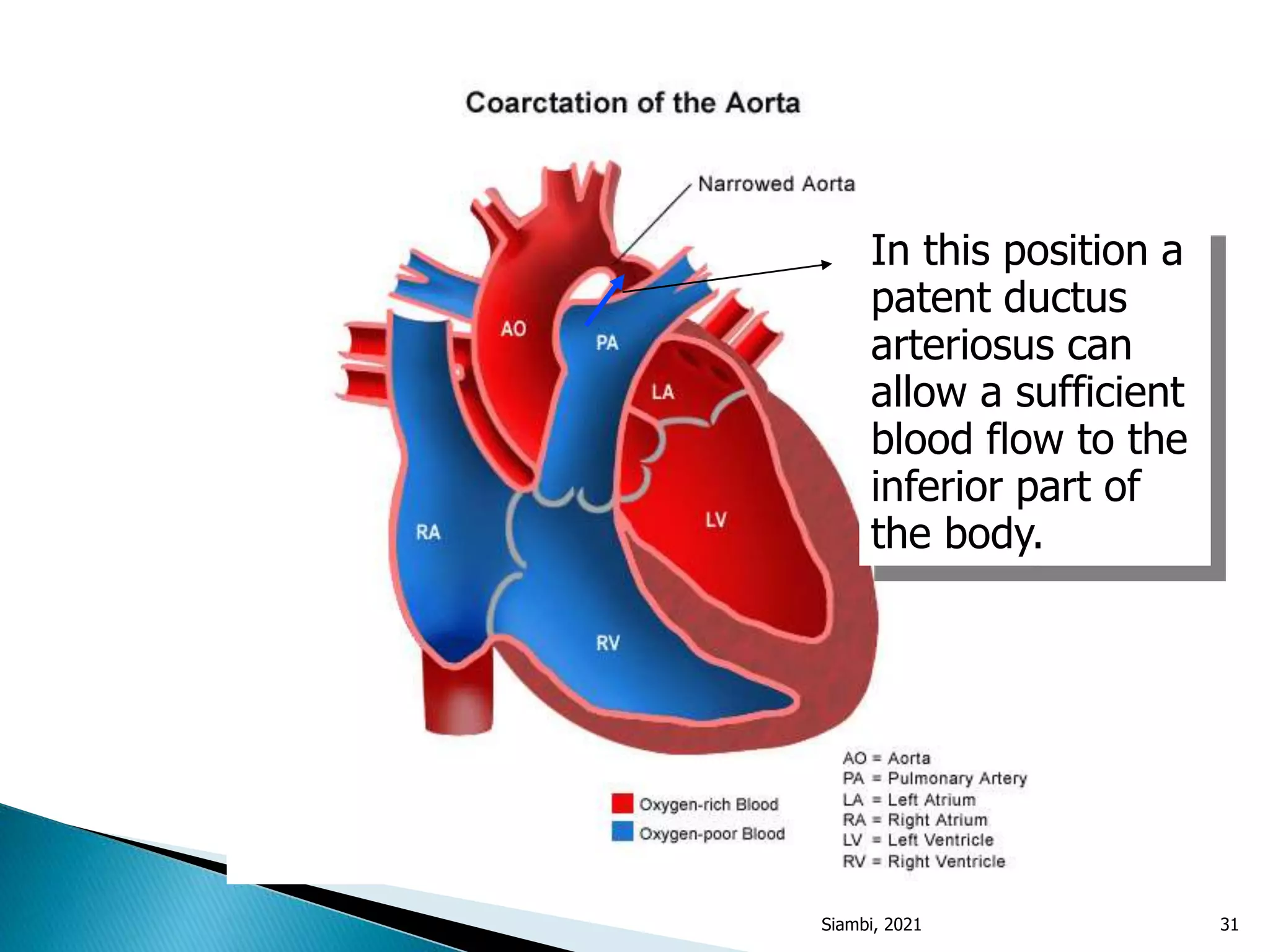
Coarctation prevalence (6% of CHD); symptoms, diagnostic tests, and treatment options presented.
Pulmonary stenosis presentation, murmur characteristics, and treatment options discussed.
Characteristics of aortic stenosis; presenting symptoms, murmurs, and treatment guidelines.
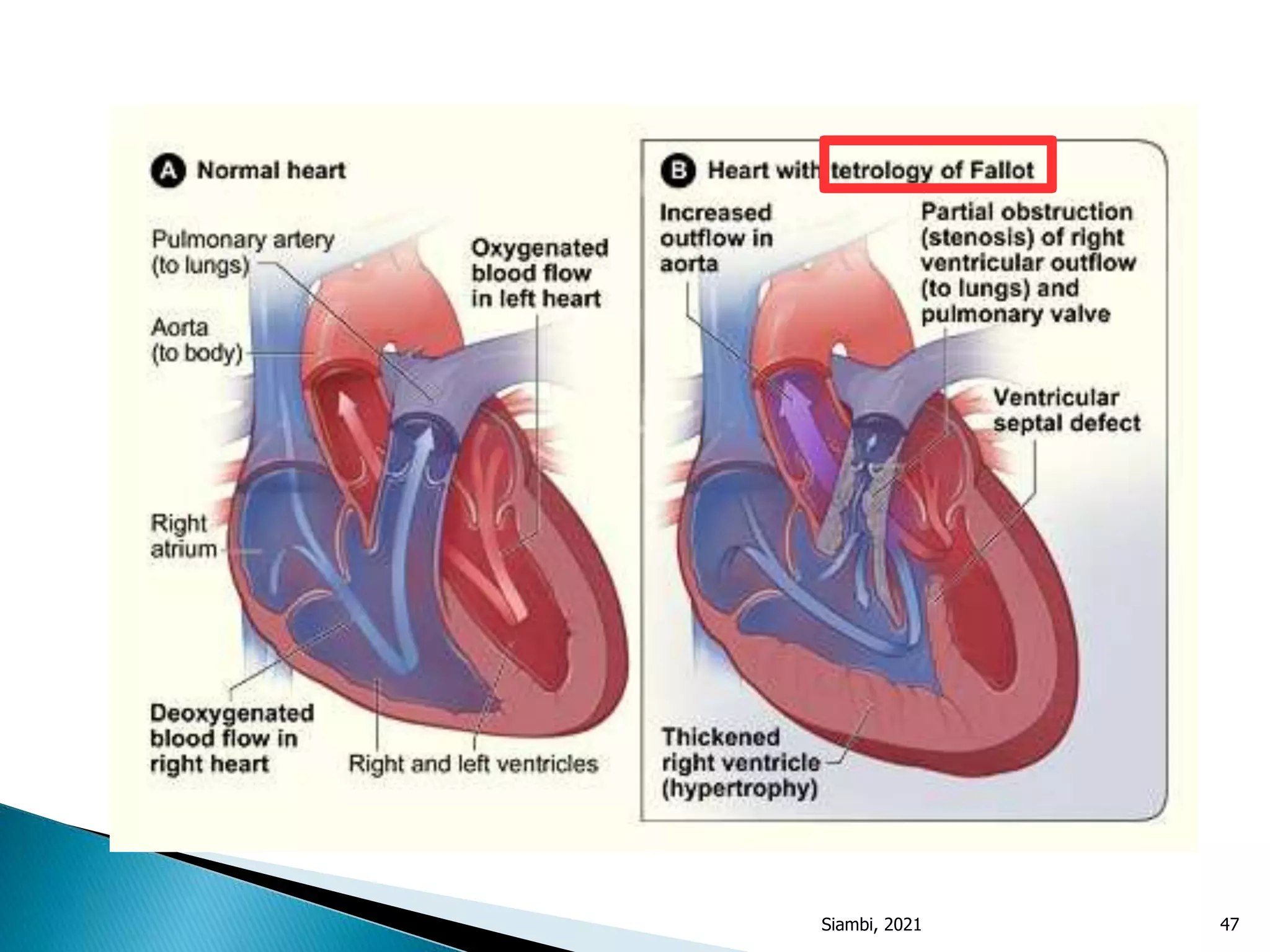
Includes TOF, tricuspid atresia; common characteristics like cyanosis and clinical findings.
Detailed management strategies including surgical interventions, symptoms, and echocardiographic findings.
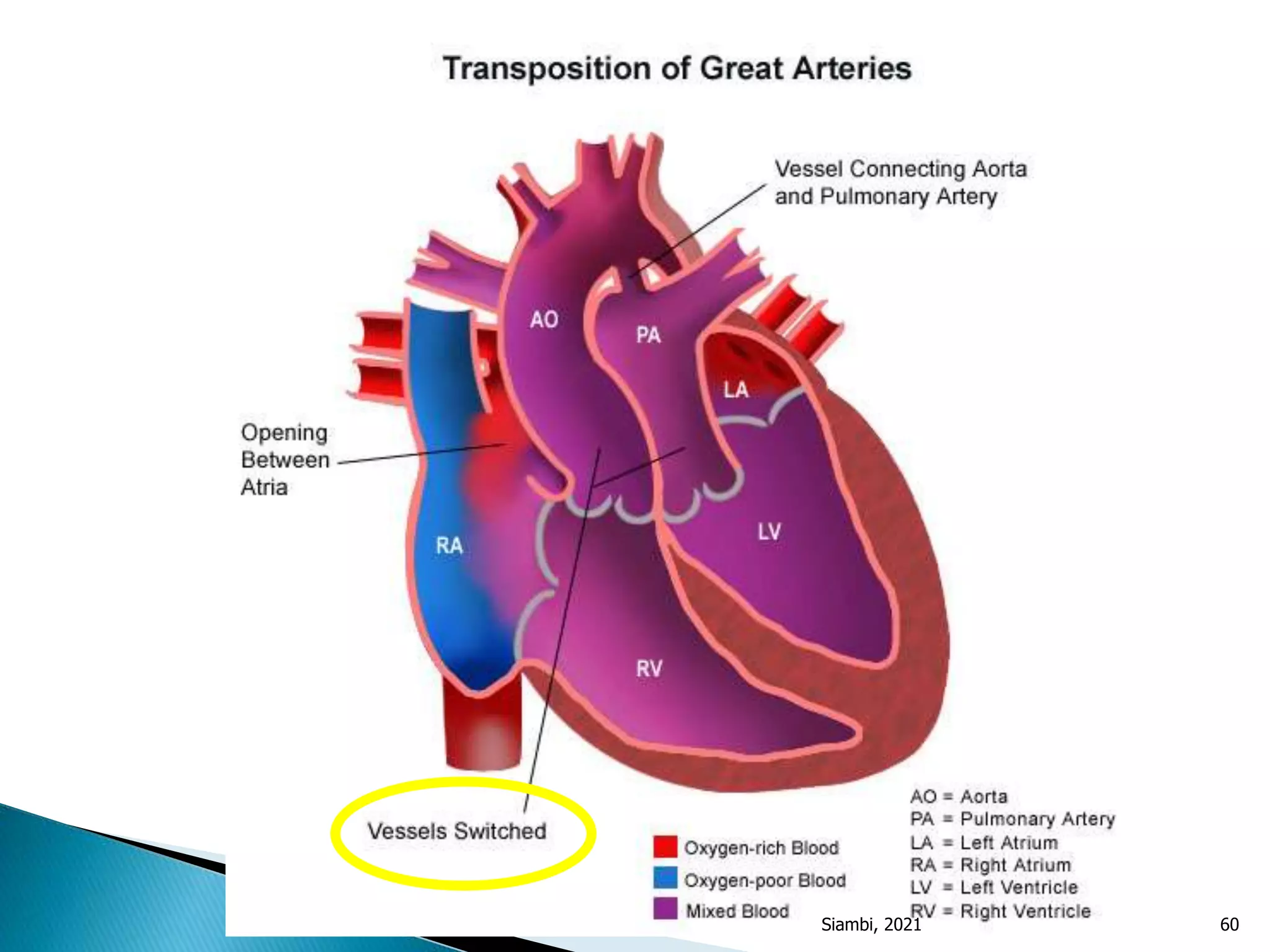
TGA is life-threatening without mixing blood; treatment with PGE1 and surgical correction discussed.
Rare condition (1% CHD); symptoms related to pulmonary hypertension and surgical intervention.
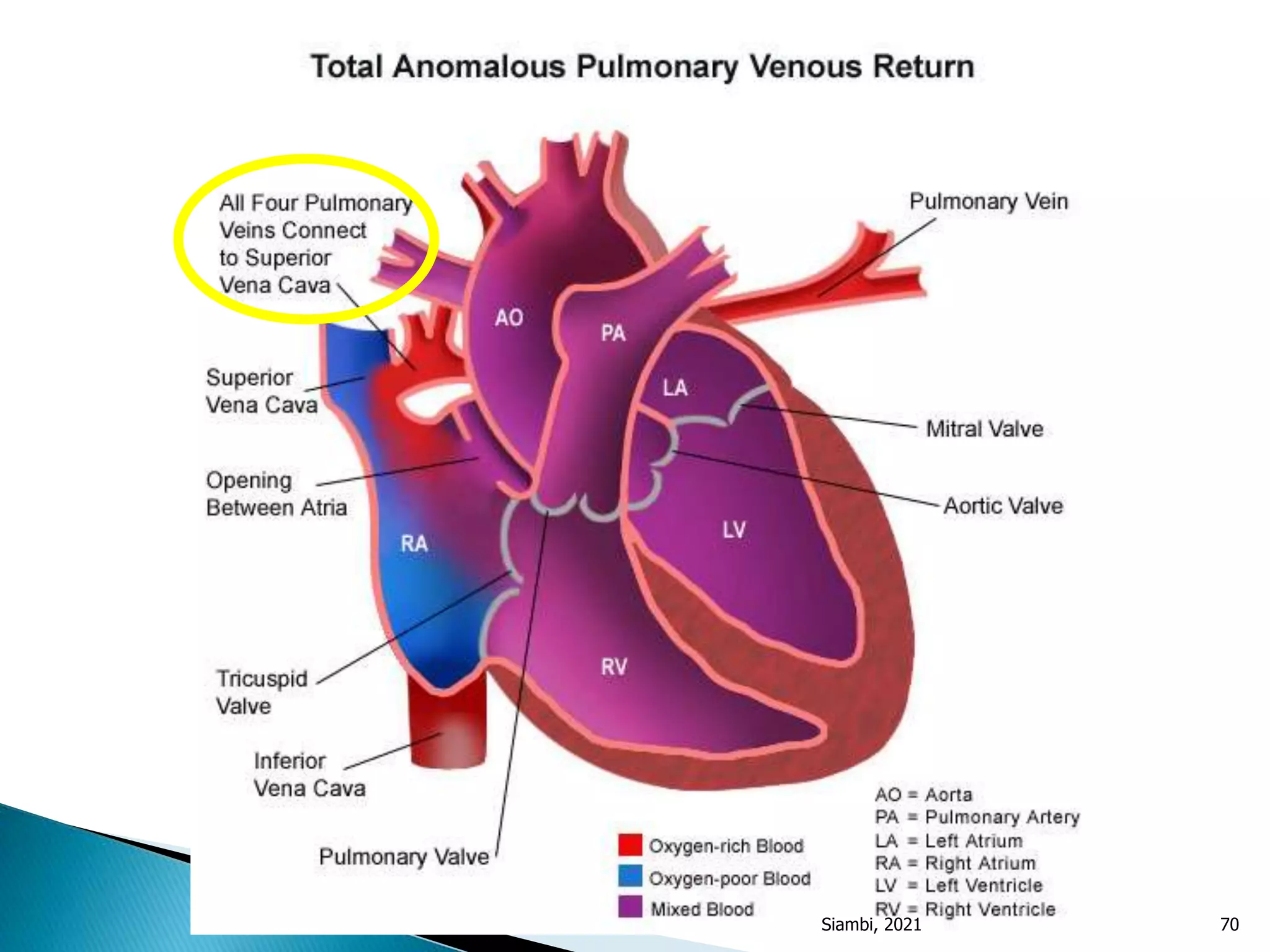
Presentation in infants, symptoms of severe illness, need for surgical correction.
Rare (1% CHD), types discussed; surgical treatment necessity in symptomatic children.
Severe hypoplasia; cardiogenic shock upon ductus closure; urgent management discussed.
Differentiating innocent murmurs from pathological; genetic, environmental causes of CHD.
Diagnostic methods: echocardiogram, ECG, imaging, and lab findings essential to pinpoint CHD.



































































