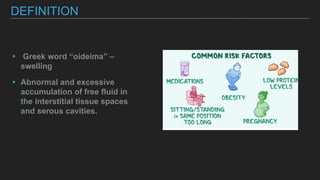
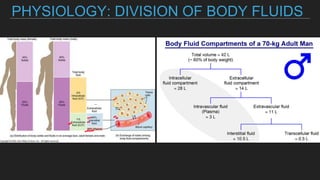
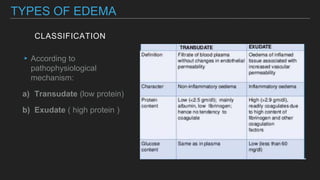
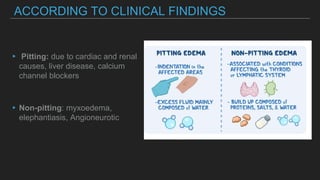
Edema is an abnormal accumulation of fluid in the interstitial spaces of tissues. It is caused by an imbalance between hydrostatic and oncotic pressures in capillaries that allows fluid to shift into tissues. Common causes include congestive heart failure, renal failure, liver disease, and lymphatic obstruction from malignancy or radiation. Edema is classified by location, protein content, pitting characteristics, and underlying cause. Treatment focuses on addressing the root cause, restricting sodium intake, bed rest, and diuretics. Follow up monitors weight, edema resolution, and input/output.