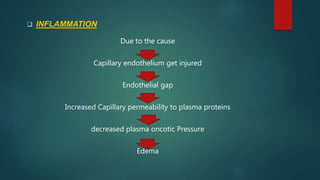
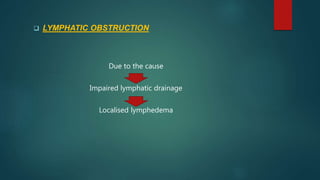
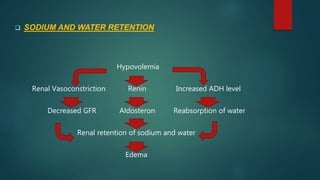
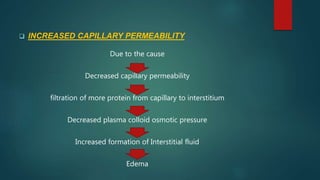
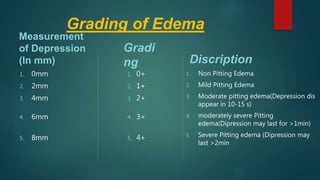
Edema is the accumulation of excess fluid in body tissues. It can be caused by increased hydrostatic pressure, reduced plasma oncotic pressure, inflammation, lymphatic obstruction, or sodium/water retention. Edema is classified as generalized, localized, pitting or non-pitting depending on location and indentation. Signs include weight gain, swelling, and distended veins. Treatment focuses on managing the underlying cause, restricting salt intake, using diuretics and antibiotics, and preventing complications through positioning, skin care, and monitoring for worsening symptoms.