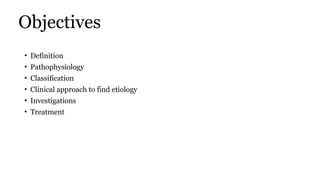
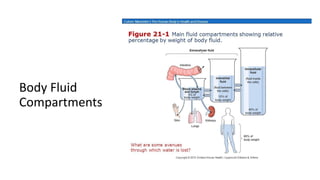
Distribution of bodywater -70kg adult
TBW
(Total Body
Water)
42L
ICF
Extra-cellular
Fluid vol
14L
ICF
Intra-cellular
Fluid vol
28L Interstitial fluid
10.5L
Plasma
3L
Transcellular fluid
4.
Definition
Edema is definedas a
Clinically apparent increase in the interstitial fluid volume, which develops when starlings forces
are altered so that there is increased flow of fluids from vascular system into the interstitium.
Accumulation of fluid in interstitial compartment
• Predominantly water
• Can contain protein and cells depending on the cause
• Minimal fluid required to clinically elicit is 4 to 5L
Extracellular fluid volume expansion is often dependent.
Ambulatory patients, edema is in the feet and lower legs;
Patients requiring bed rest develop edema in the buttocks, genitals, and posterior thighs.
• Women who lie on only one side may develop edema in the dependent breast.
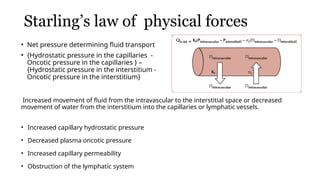
Starling’s law ofphysical forces
• Net pressure determining fluid transport
• {Hydrostatic pressure in the capillaries -
Oncotic pressure in the capillaries } –
{Hydrostatic pressure in the interstitium -
Oncotic pressure in the interstitium}
Increased movement of fluid from the intravascular to the interstitial space or decreased
movement of water from the interstitium into the capillaries or lymphatic vessels.
• Increased capillary hydrostatic pressure
• Decreased plasma oncotic pressure
• Increased capillary permeability
• Obstruction of the lymphatic system
7.
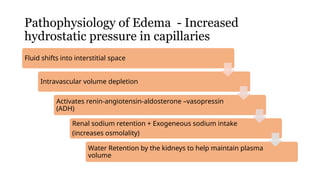
Pathophysiology of Edema- Increased
hydrostatic pressure in capillaries
Fluid shifts into interstitial space
Intravascular volume depletion
Activates renin-angiotensin-aldosterone –vasopressin
(ADH)
Renal sodium retention + Exogeneous sodium intake
(increases osmolality)
Water Retention by the kidneys to help maintain plasma
volume
8.
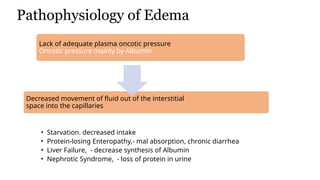
Pathophysiology of Edema
•Starvation. decreased intake
• Protein-losing Enteropathy,- mal absorption, chronic diarrhea
• Liver Failure, - decrease synthesis of Albumin
• Nephrotic Syndrome, - loss of protein in urine
Lack of adequate plasma oncotic pressure
Oncotic pressure mainly by Albumin
Decreased movement of fluid out of the interstitial
space into the capillaries
9.
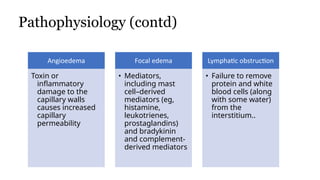
Pathophysiology (contd)
Angioedema
Toxin or
inflammatory
damageto the
capillary walls
causes increased
capillary
permeability
Focal edema
• Mediators,
including mast
cell–derived
mediators (eg,
histamine,
leukotrienes,
prostaglandins)
and bradykinin
and complement-
derived mediators
Lymphatic obstruction
• Failure to remove
protein and white
blood cells (along
with some water)
from the
interstitium..
10.
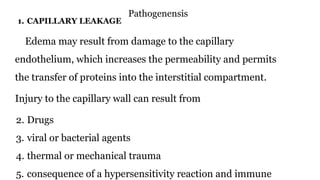
Pathogenensis
1. CAPILLARY LEAKAGE
Edemamay result from damage to the capillary
endothelium, which increases the permeability and permits
the transfer of proteins into the interstitial compartment.
Injury to the capillary wall can result from
2. Drugs
3. viral or bacterial agents
4. thermal or mechanical trauma
5. consequence of a hypersensitivity reaction and immune
11.
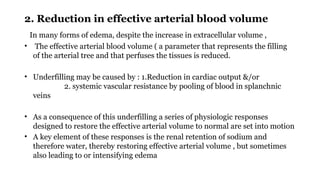
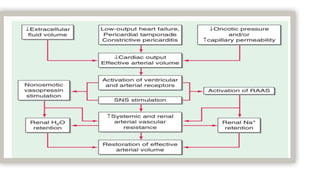
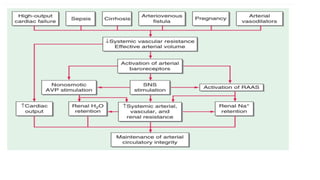
2. Reduction ineffective arterial blood volume
In many forms of edema, despite the increase in extracellular volume ,
• The effective arterial blood volume ( a parameter that represents the filling
of the arterial tree and that perfuses the tissues is reduced.
• Underfilling may be caused by : 1.Reduction in cardiac output &/or
2. systemic vascular resistance by pooling of blood in splanchnic
veins
• As a consequence of this underfilling a series of physiologic responses
designed to restore the effective arterial volume to normal are set into motion
• A key element of these responses is the renal retention of sodium and
therefore water, thereby restoring effective arterial volume , but sometimes
also leading to or intensifying edema
14.
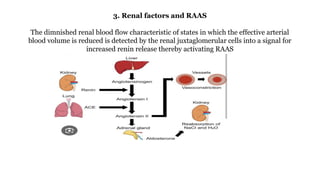
3. Renal factorsand RAAS
The dimnished renal blood flow characteristic of states in which the effective arterial
blood volume is reduced is detected by the renal juxtaglomerular cells into a signal for
increased renin release thereby activating RAAS
15.
4. Arginine vasopressin
Thesecretion of arginine vasopressin (AVP) occurs in
response to increased intracellular osmolar concentration.
↓
V2 receptor stimulation
↓
AVP increases the reabsorption of water from distal tubule
and collecting ducts of kidney
↓
Increase in total body water
16.
5. Endothelin 1
•This is a potent vasoconstrictor released by endothelial cells.
• Its concentration in the plasma is elevated in patients with severe heart
failure leading to renal vasoconstriction , sodium retention and edema
17.
Natriuretic peptides
– Ventriculardiastolic pressure rises
– ANP and BNP released
– Binds to natriuretic receptor A
– Excretion of Na and water by augmenting GFR , inhibits Na absorption
in the PCT , and inhibiting release of renin and aldosterone
– Leading to dilatation of arterioles and venules by antagonising
AII ,AVP, and sympathetic stimulation.
– Although circulating levels of ANP and BNP increases in heart failure
and cirrhosis they are not sufficiently potent to prevent edema
formation.
20.
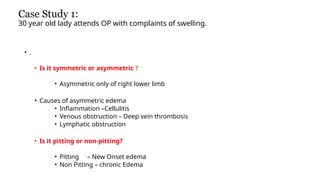
Case Study 1:
30year old lady attends OP with complaints of swelling.
• .
• Is it symmetric or asymmetric ?
• Asymmetric only of right lower limb
• Causes of asymmetric edema
• Inflammation –Cellulitis
• Venous obstruction – Deep vein thrombosis
• Lymphatic obstruction
• Is it pitting or non-pitting?
• Pitting – New Onset edema
• Non Pitting – chronic Edema
21.
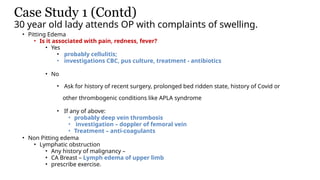
Case Study 1(Contd)
30 year old lady attends OP with complaints of swelling.
• Pitting Edema
• Is it associated with pain, redness, fever?
• Yes
• probably cellulitis;
• investigations CBC, pus culture, treatment - antibiotics
• No
• Ask for history of recent surgery, prolonged bed ridden state, history of Covid or
other thrombogenic conditions like APLA syndrome
• If any of above:
• probably deep vein thrombosis
• investigation – doppler of femoral vein
• Treatment – anti-coagulants
• Non Pitting edema
• Lymphatic obstruction
• Any history of malignancy –
• CA Breast – Lymph edema of upper limb
• prescribe exercise.
22.
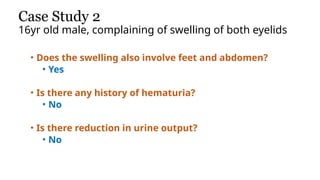
Case Study 2
16yrold male, complaining of swelling of both eyelids
• Does the swelling also involve feet and abdomen?
• Yes
• Is there any history of hematuria?
• No
• Is there reduction in urine output?
• No
23.
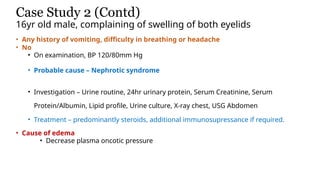
Case Study 2(Contd)
16yr old male, complaining of swelling of both eyelids
• Any history of vomiting, difficulty in breathing or headache
• No
• On examination, BP 120/80mm Hg
• Probable cause – Nephrotic syndrome
• Investigation – Urine routine, 24hr urinary protein, Serum Creatinine, Serum
Protein/Albumin, Lipid profile, Urine culture, X-ray chest, USG Abdomen
• Treatment – predominantly steroids, additional immunosupressance if required.
• Cause of edema
• Decrease plasma oncotic pressure
24.
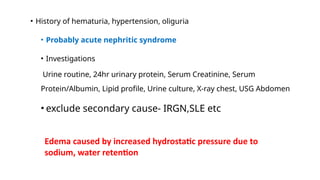
• History ofhematuria, hypertension, oliguria
• Probably acute nephritic syndrome
• Investigations
Urine routine, 24hr urinary protein, Serum Creatinine, Serum
Protein/Albumin, Lipid profile, Urine culture, X-ray chest, USG Abdomen
• exclude secondary cause- IRGN,SLE etc
Edema caused by increased hydrostatic pressure due to
sodium, water retention
25.
Case Study 3
60yrold male, complaining of swelling of feet
• History of diabetes melitus of 5yr duration,
History of hypertension for which he is taking amlodipin.
• Is he ever told to have proteinuria
• No
• Does he have history of treatment for Diabetic Retinopathy
• No
• Urine routine – normal. No microalbuminuria
• Renal profile – normal
• Probable cause – Amolodipin induced edema
• Exclude hypothyroidism
26.
Case Study 4
40yrold alcoholic with history of jaundice presents with
distension of abdomen and edema of feet.
• Any history of fever, abdominal pain, diarrhea, reduction
in urine output
• No
• Is he jaundiced
• No
• Investigation – Urine Routine, LFT, Renal profile
• Investigation shows hypoalbuminemia
• Probable cause – decreased oncotic pressure
27.
Case Study 5
70yrold gentleman presents with difficulty in breathing and edema
• History of chest pain - Yes
• Suggestive of coronary disease
• History of hypertension
• Hypertensive left ventricular failure
• Renal Profile investigation show increased Creatinine 5mg
• Probable cause – acute pulmonary edema due to fluid overload and acute left
ventricular failure
• Increased hydrostatic pressure leading to salt and water retention aggravated by
kidney failure
28.
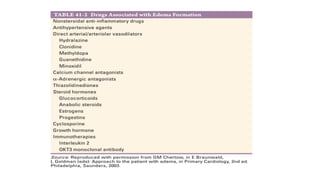
Miscellaneous cause
• Idiopathicedema
• This is usually seen in females maybe pre-menstrual or no
obvious cause
• Hypothyroidism
29.
Red Flags
• Suddenonset
• Significant pain
• Shortness of breath
• Fever
• History of a heart disorder or an abnormal cardiac examination
• Haemoptysis, dyspnea, or pleural friction rub
• Hepatomegaly, jaundice, ascites, splenomegaly, or hematemesis
• Unilateral leg swelling with tenderness
30.
Evaluation of edema
Patientswith generalized edema,
Urine routine, - Alb/cr ratio, microscopic hematuria
complete blood count (CBC), blood urea creatinine,
serum electrolytes,serum protein –Albumin
Special investigations,
Brain natriuretic peptide (BNP) for suspected heart failure
D-dimer for suspected pulmonary embolism.
• Patients with isolated lower-extremity swelling
Ultrasonography.,Doppler
• Treatment of Edema
31.
Treatment
• eatment ofEdema
Identify specific cause and treat
⮚ Dietary Restriction Of Dietary Sodium.
⮚ Advanced Cirrhosis Or Nephrotic Syndrome -Severe Sodium Restriction ( 1 G/Day).
≤
⮚ Potassium Salts Are Often Substituted For Sodium Salts To Make Sodium Restriction Tolerable;
⮚ Caution In Patients Receiving Potassium-sparing Diuretics, Angiotensin-converting Enzyme
(Ace) Inhibitors, Or Angiotensin Ii Receptor Blockers (Arbs) And In Those With A Kidney Disorder
Because Potentially Fatal Hyperkalemia Can Result.
32.
In patients withheart failure or nephrotic syndrome
with or without diabetes
⮚ Sodium-glucose cotransporter 2 (SGLT2) inhibitors
(eg, canagliflozin, dapagliflozin, empagliflozin)
⮚ lower serum glucose in patients with diabetes
⮚ induce diuresis by increasing natriuresis and glycosuria without
significantly affecting serum electrolytes
33.
Treatment (contd)
Loop orthiazide diuretics. ,
monitor for hypokalemia
potassium-sparing diuretics
monitor for hyperkalemia
Combine Thiazides with potassium sparing diuretics
34.
Precautions in elderlywhen drugs are used for
edema
• Starting doses low and evaluating patients thoroughly when the dose is changed
• Monitoring for orthostatic hypotension if diuretics, ACE inhibitors, angiotensin
II receptor blockers, or beta-blockers are used
• Frequently testing for hypokalemia or hyperkalemia
• Not stopping calcium channel blockers because of pedal edema, which is benign
• monitoring daily weight helps in monitoring clinical improvement or deterioration
immensely.
• Key Points
35.
Take home messge
•Generalised edema- CLD, HEART Failure, Renal disease
• Localised edema – Exclude local causes – venous
obstruction, lymphatic obstruction, infection
• Acute onset edema – detailed evaluation
• Treatment depends on the cause































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)











![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)




