Download to read offline





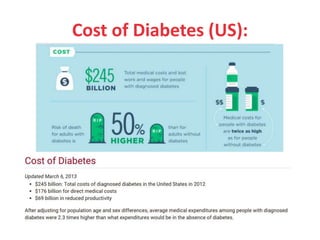


























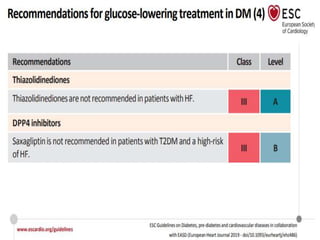

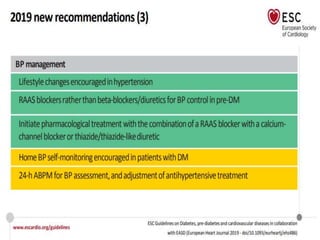





































Diabetes Mellitus was defined as a metabolic disease caused by the body's inability to produce insulin or enough insulin, leading to elevated blood glucose levels. Symptoms of diabetes were discussed. Prediabetes was associated with increased cardiovascular risk, so screening and treatment of modifiable risk factors is suggested. Lifestyle interventions and metformin were shown to reduce progression to diabetes in those with prediabetes. The document provided recommendations on physical activity, smoking cessation, metabolic surgery, cardiovascular disease screening and treatment, and management of hypoglycemia and diabetic ketoacidosis.



































































