Downloaded 20 times
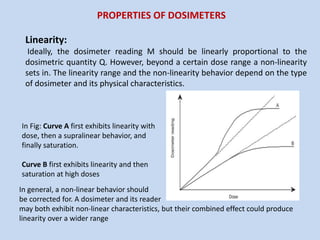
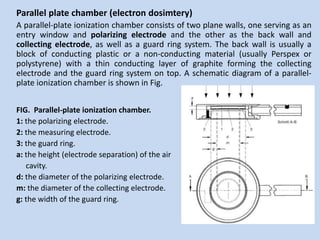
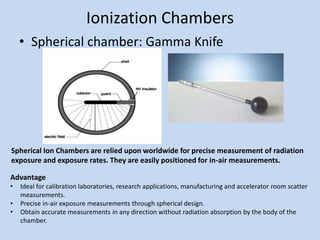
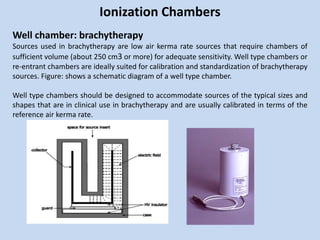
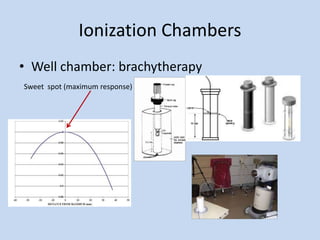
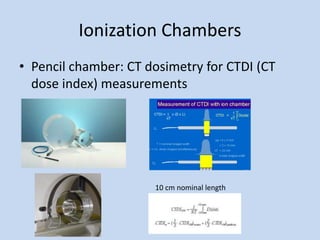
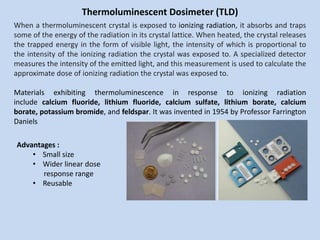
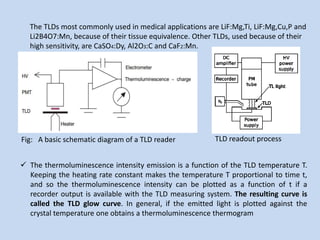
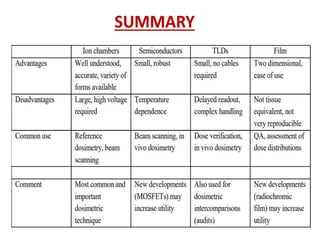


This document discusses different types of radiation dosimeters, including their properties, uses, and limitations. It focuses on ionization chamber dosimetry systems, describing cylindrical thimble chambers, parallel plate chambers, spherical chambers, well chambers, and pencil chambers. It also discusses thermoluminescent dosimeters (TLD), noting that TLD crystals absorb and trap radiation energy then emit light when heated, allowing dose measurement. The document provides an overview of key factors such as linearity, dose rate dependence, energy dependence, and directional dependence for dosimeters.



































































