1) Competency-based medical education (CBME) is an outcomes-based approach that uses competencies as an organizing framework for designing, implementing, assessing, and evaluating medical education programs.
2) Traditional medical education focuses on knowledge acquisition with a fixed length and variable outcomes, while CBME emphasizes knowledge application with a variable length and defined outcomes.
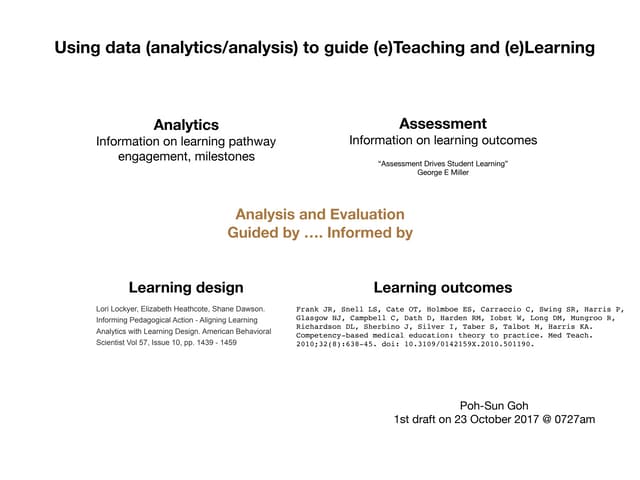
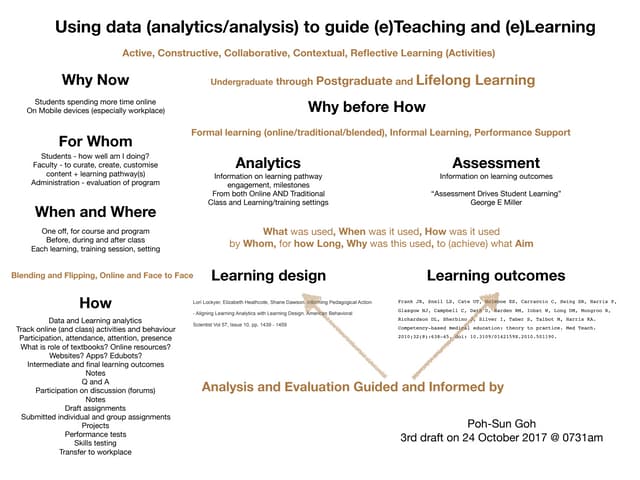
3) Effective assessment in CBME uses a variety of objective measurement tools aligned with outcomes, incorporates direct observation and authentic tasks, and emphasizes formative assessment to drive future learning.




















































![AETCOM [ATTITUDE,ETHICS & COMMUNICATION IN MEDICAL EDUCATION] EDUCATION](https://cdn.slidesharecdn.com/ss_thumbnails/aetconnewpppt-200525080043-thumbnail.jpg?width=640&height=640&fit=bounds)