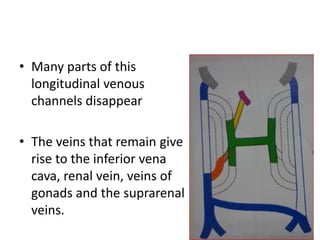
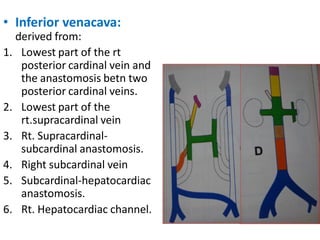
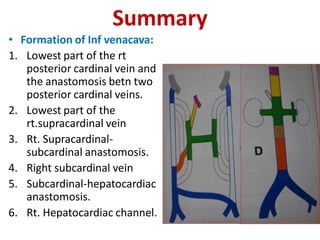
1. The inferior vena cava forms from remnants of the right posterior cardinal vein, right supracardinal vein, and connections between the right subcardinal and hepatocardiac veins.
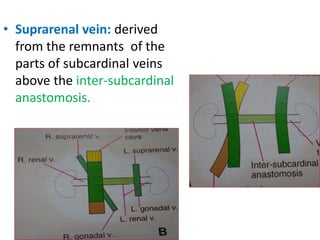
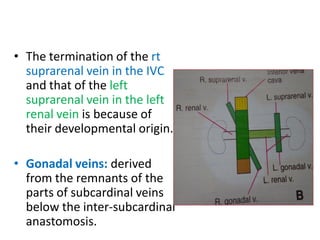
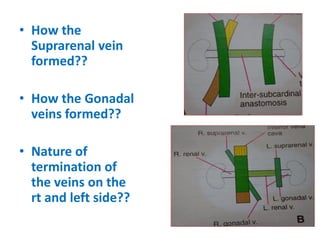
2. The suprarenal veins are derived from remnants of the subcardinal veins above the inter-subcardinal anastomosis, and the gonadal veins are derived from remnants below the inter-subcardinal anastomosis.
3. The termination of the right suprarenal vein in the inferior vena cava and the left suprarenal vein in the left renal vein results from their developmental origins in the subcardinal veins.
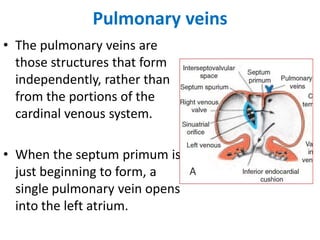
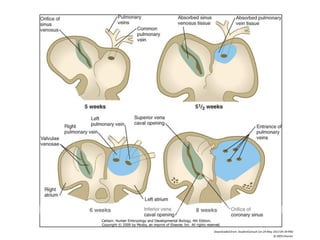
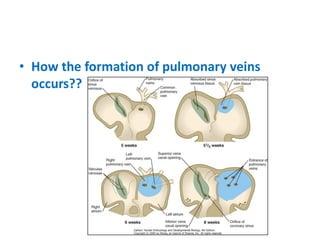
Initially, the pulmonary vein opens as a single vessel into