



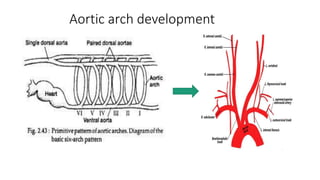

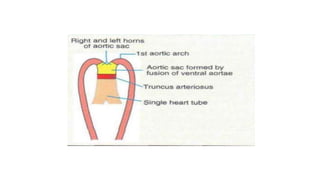
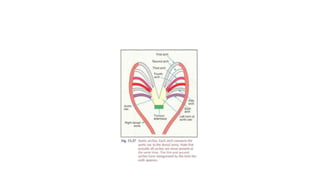







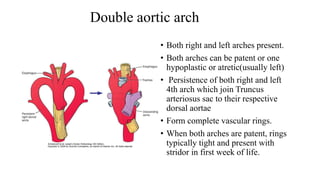


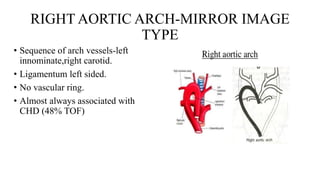
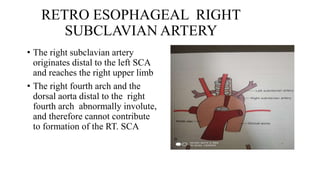



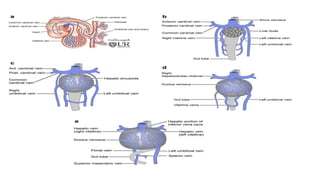

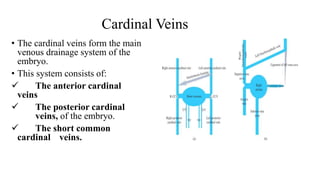



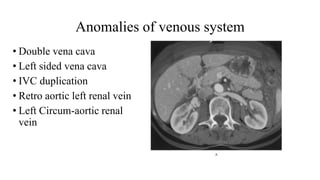





The document summarizes the development of the aortic arch, thoracic and abdominal aorta, and venous system during embryogenesis. It describes how the paired dorsal aortas fuse to form the descending aorta and how the aortic arches give rise to major arteries like the carotid and subclavian arteries. Common aortic arch anomalies are discussed along with the regression of embryonic veins and formation of major veins like the inferior vena cava from segments including the vitelline, umbilical, and cardinal veins. Rare anomalies of the venous system and arterial variations are also mentioned.























































































