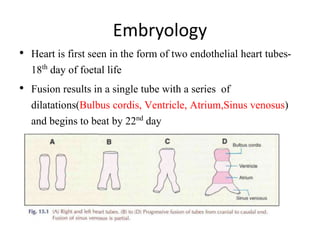
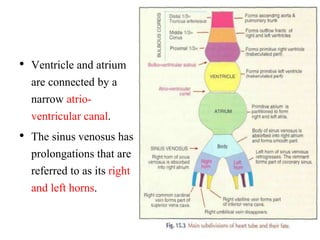
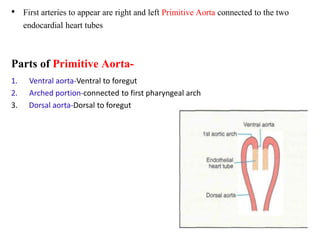
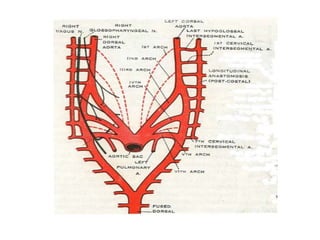
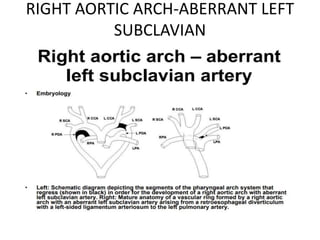
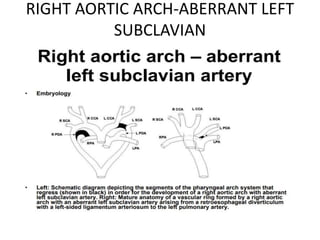
1. The aortic arches develop from the primitive aorta and pharyngeal arch arteries during embryonic development.
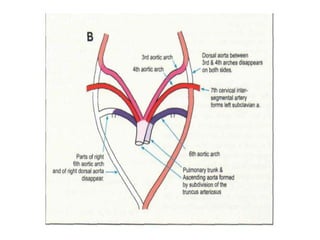
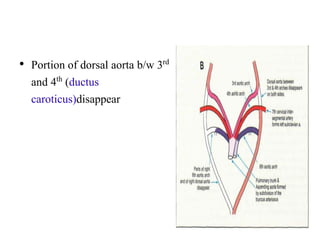
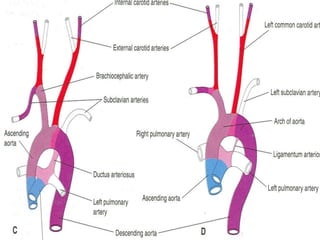
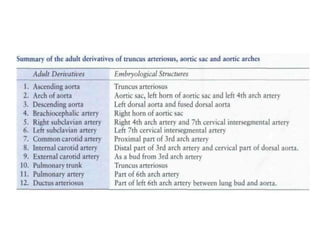
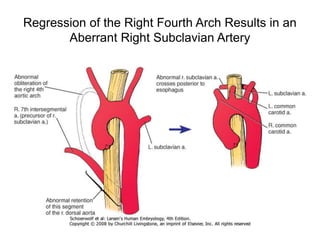
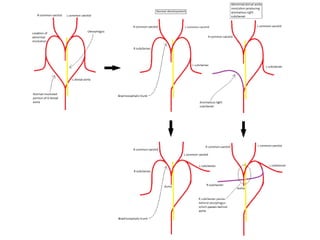
2. The right and left 3rd aortic arches normally form the common carotid arteries, while the 4th arches form the subclavian arteries.
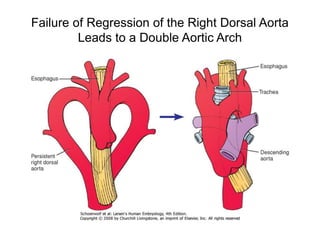
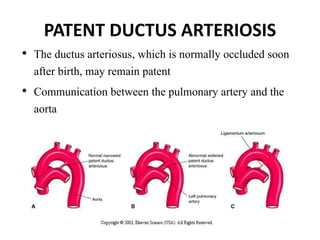
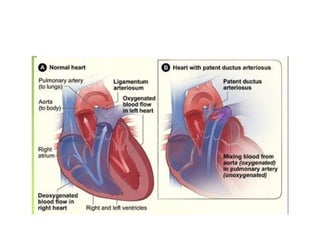
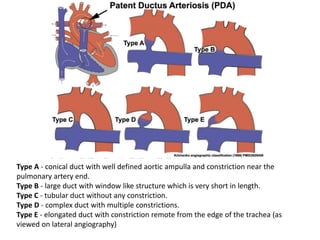
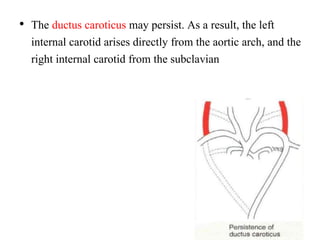
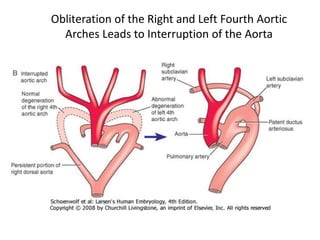
3. A number of anomalies can occur if parts of the arches fail to regress as normal or persist that typically regress. This includes double aortic arch, right aortic arch, patent ductus arteriosus, and interrupted aortic arch.
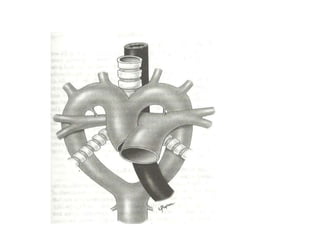
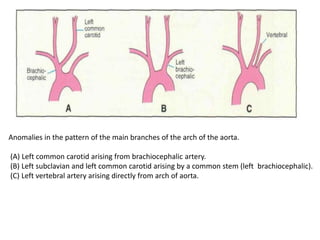
4. Proper development and regression of the aortic arches is required for normal formation of the branches of the aortic arch.




























































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)
![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)







