Downloaded 176 times
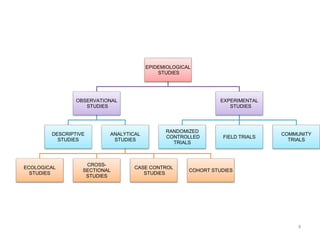
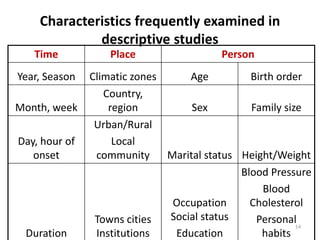


Descriptive epidemiology studies observe the distribution of diseases in populations to identify characteristics associated with diseases. This presentation discusses descriptive epidemiology, including its uses and procedures. Descriptive studies first define the population and disease, then describe disease distribution by time, place and person. This involves measuring disease prevalence and incidence and comparing rates between groups. Observing these characteristics can provide clues to disease causes and help form hypotheses about risk factors. Descriptive epidemiology provides data on disease burdens to aid health planning, research and evaluation of interventions.


















































































