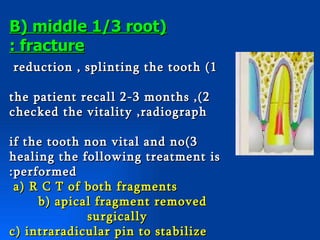
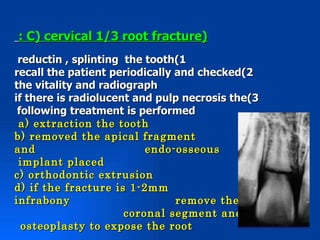
This document provides information on dental trauma, including definitions, causes, diagnosis, classification, and treatment. It begins with defining dental injury as damage limited to the teeth and supporting alveolar structures. Boys are more likely to experience dental trauma than girls. Causes include traffic accidents, falls, seizures, and sports injuries. Diagnosis involves examining the history, clinically examining soft tissues and teeth, and obtaining radiographs. Injuries are classified based on their severity and specific treatments are outlined for each class.