Download to read offline
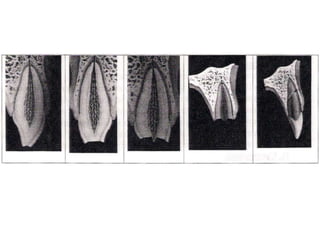


This document provides information on the management and treatment of traumatic dental injuries in children. It discusses the diagnosis process, which involves taking a medical and dental history, performing a clinical examination, conducting sensitivity tests, and getting radiographs. The clinical exam evaluates soft tissues, hard tissues, tooth displacement, mobility, fractures, and color changes. Treatment depends on the specific injury and may include protecting soft tissues, monitoring concussed teeth, splinting subluxated teeth, restoring tooth fractures with calcium hydroxide, crowns, or composite resins, and reattaching tooth fragments when possible. The goal is to restore function and aesthetics while protecting the pulp.























































































