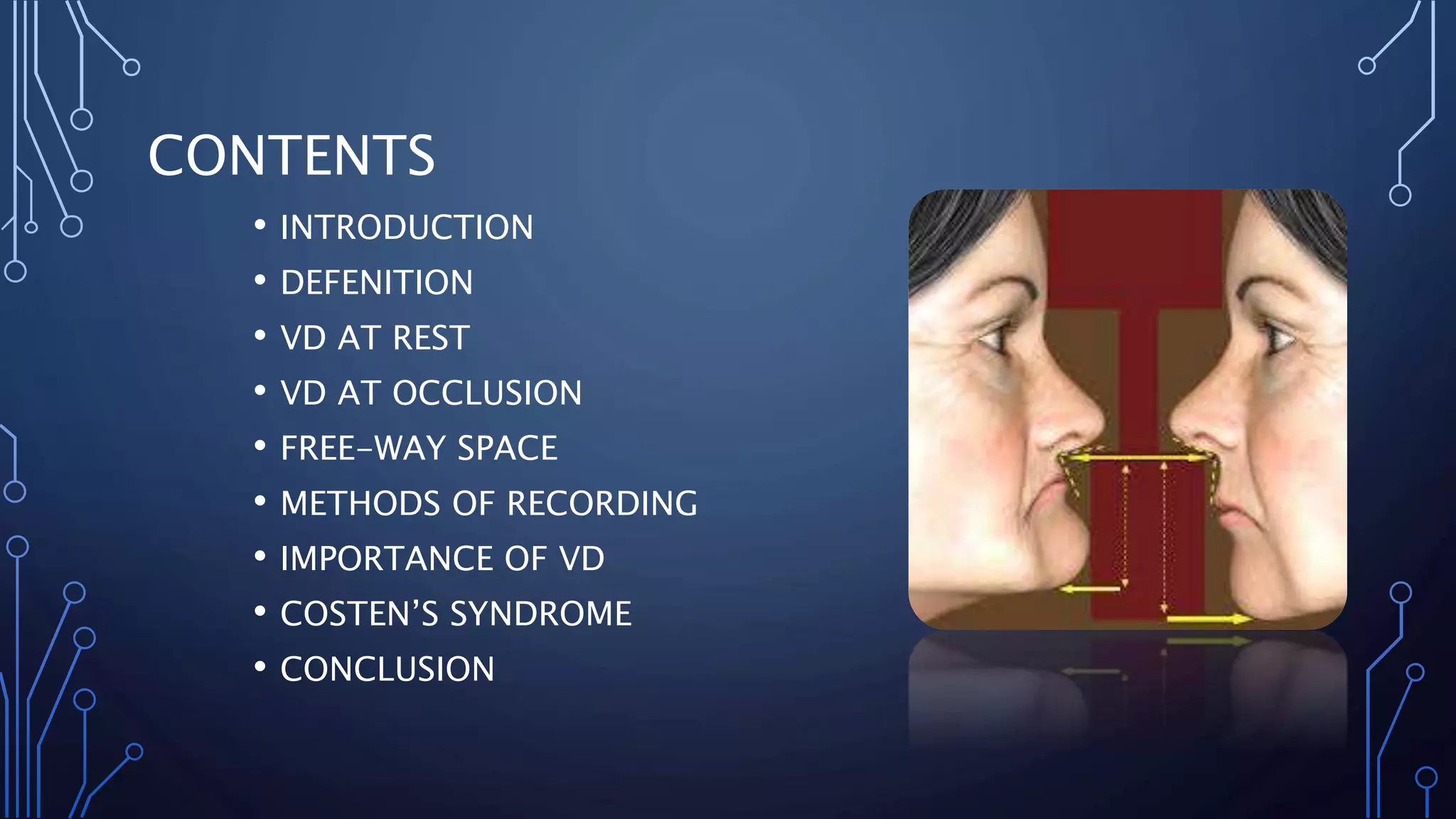
The document discusses vertical dimension (VD), which is the amount of separation between the maxilla and mandible. It defines VD at rest and VD at occlusion, and describes several methods for measuring each, including facial measurements, anatomic landmarks, tactile sense, and the use of occlusal rims. Maintaining the proper VD is important as changes can cause discomfort, strain, or Costen's Syndrome. The document concludes that while no single method is best, using multiple techniques can help verify the correct VD.






































































![vertical jaw relation [Autosaved].pptx .](https://cdn.slidesharecdn.com/ss_thumbnails/verticaljawrelationautosaved-250920192706-cb5ca831-thumbnail.jpg?width=640&height=640&fit=bounds)





























