Downloaded 171 times



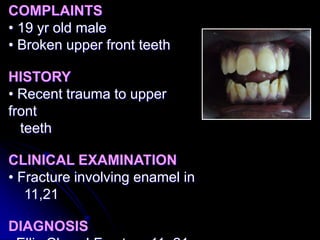







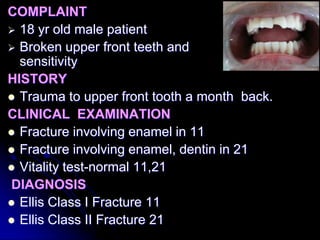


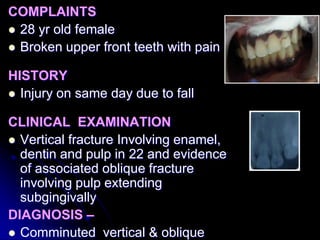





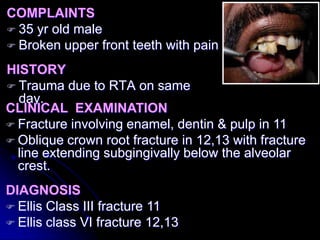



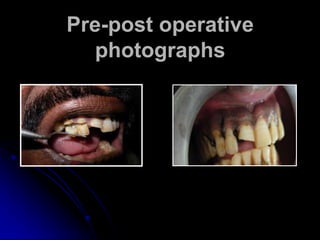








This document discusses various case reports of anterior tooth fractures treated with different techniques. It describes 5 cases: 1) enameloplasty to reshape a fractured enamel surface; 2) reattachment of a fractured fragment using composite resin; 3) laminate restoration with glass ionomer cement and composite for a fracture involving enamel and dentin; 4) management of a vertical fracture involving pulp using orthodontic banding and post-core buildup; and 5) surgical reattachment of fractured fragments involving pulp. The document discusses advantages of reattachment techniques and highlights factors like prognosis and esthetics. It emphasizes the importance of restoring smiles and improving patients' quality of life.



































































