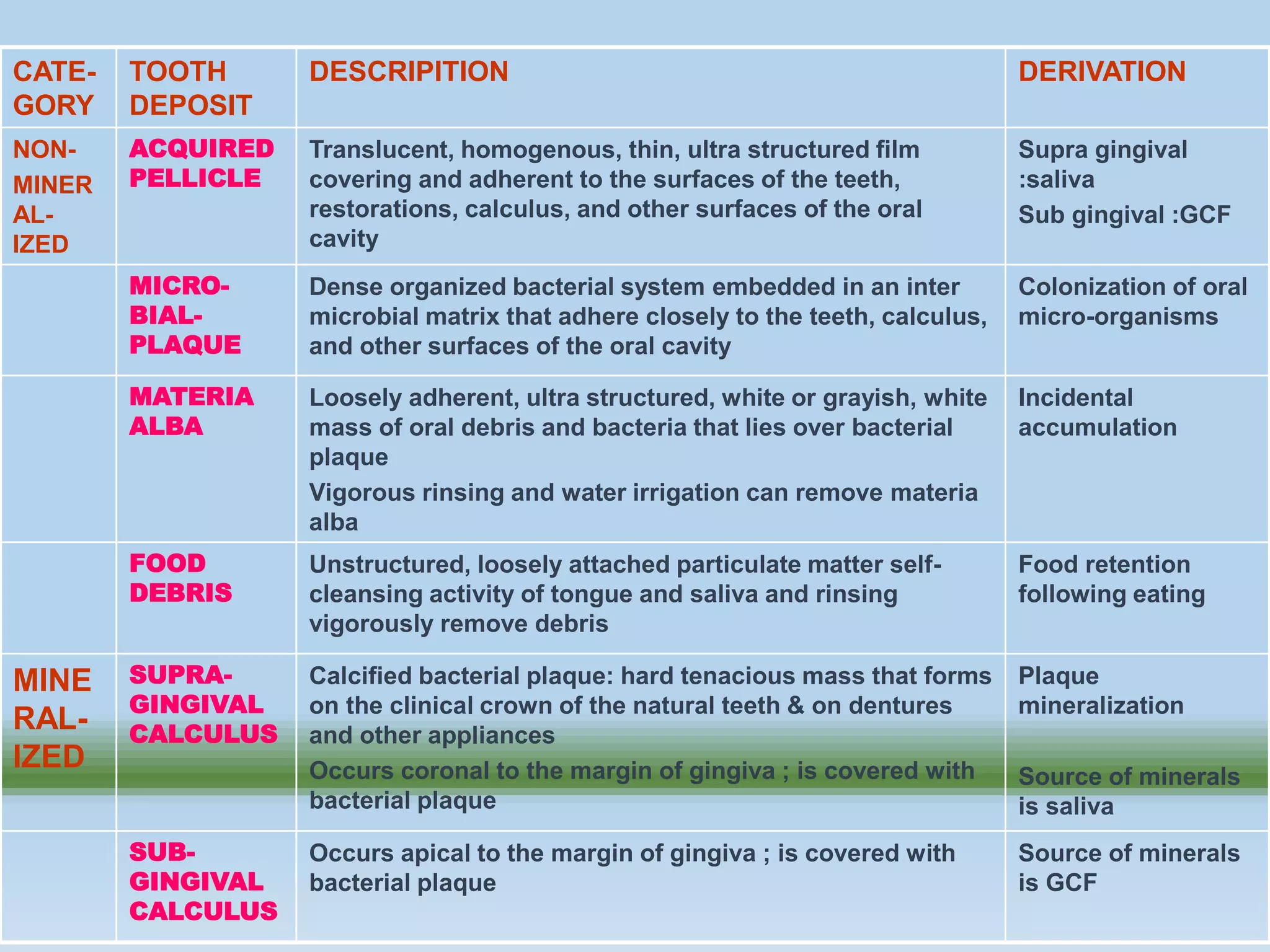



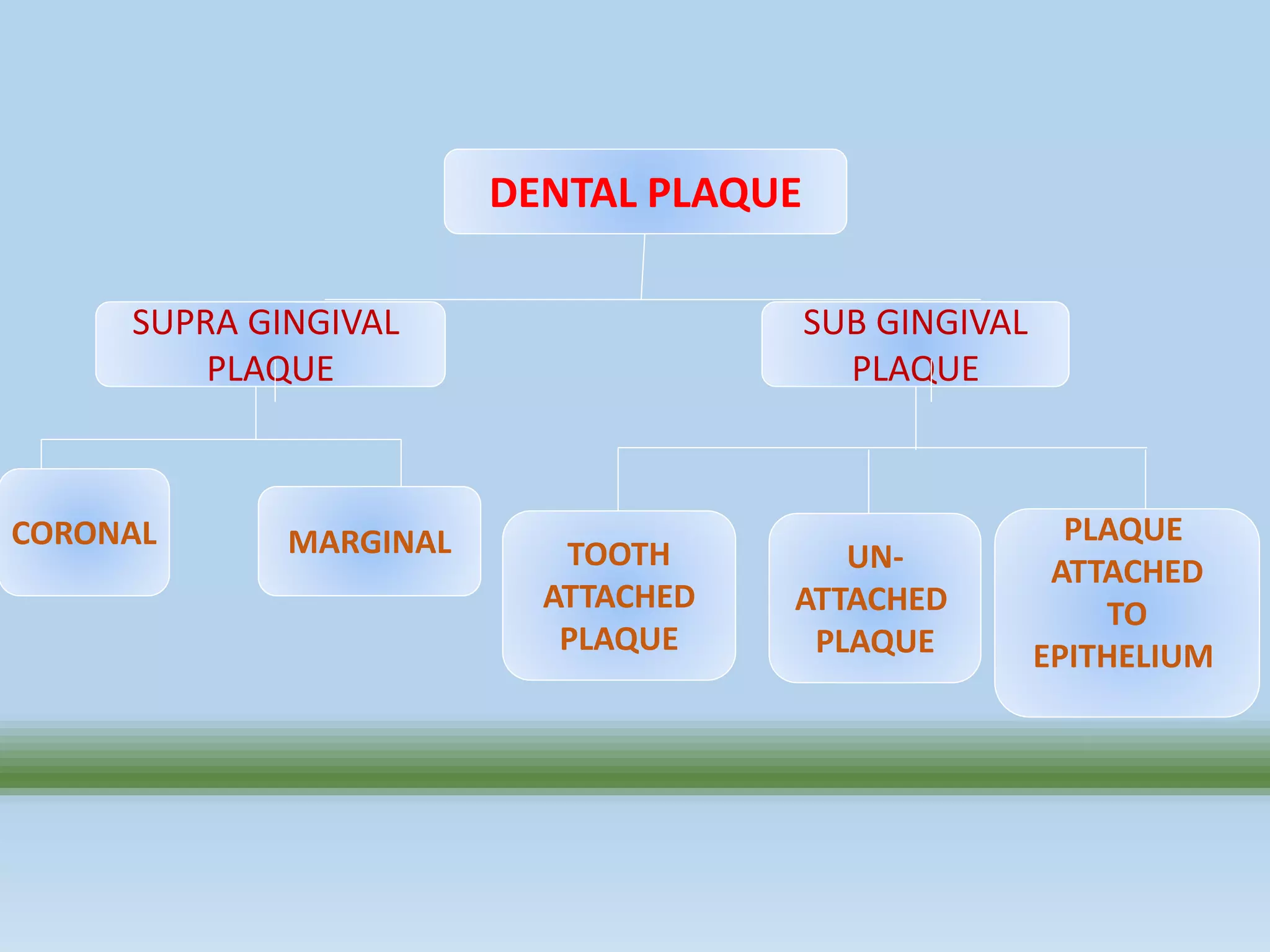

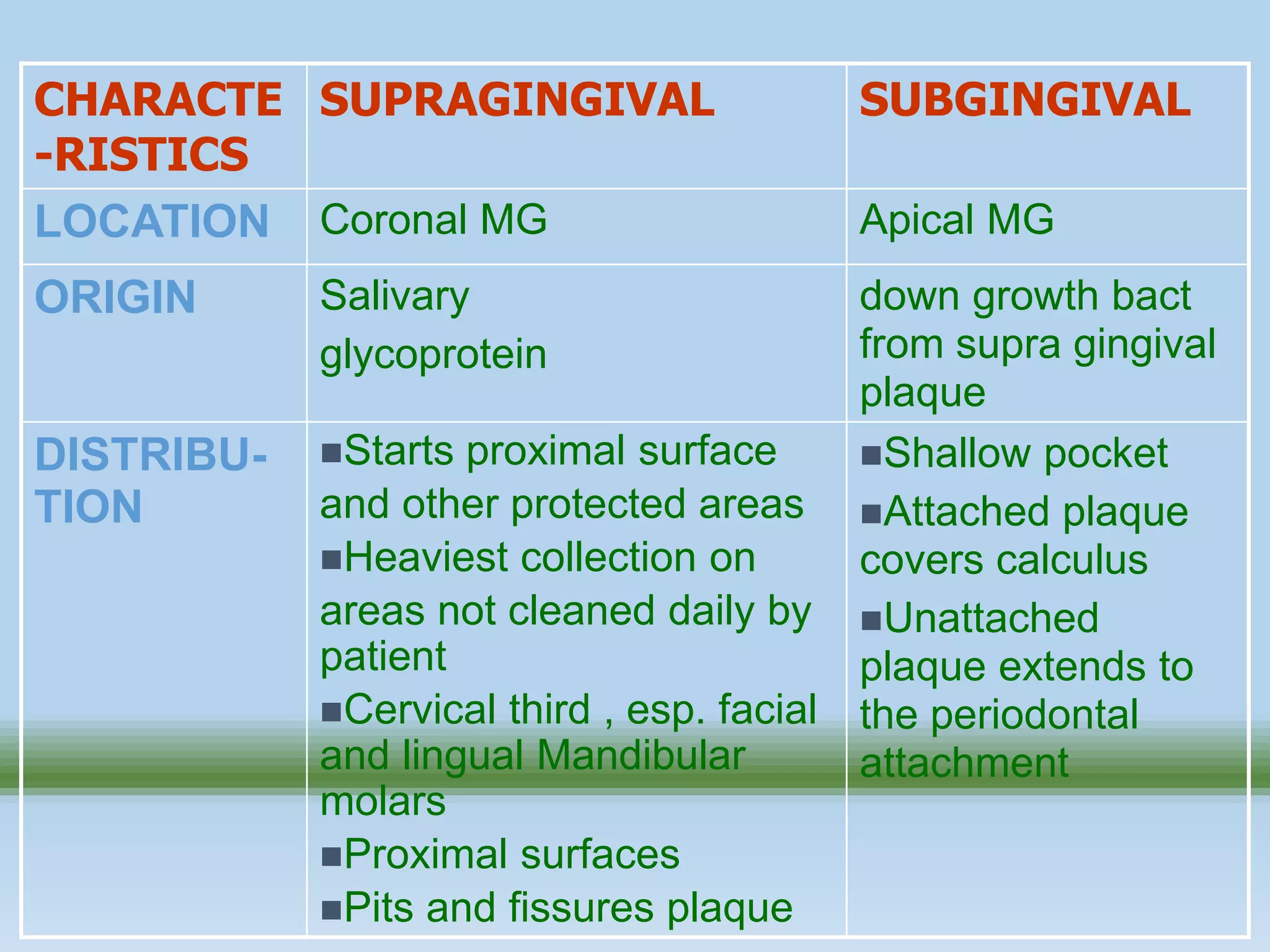


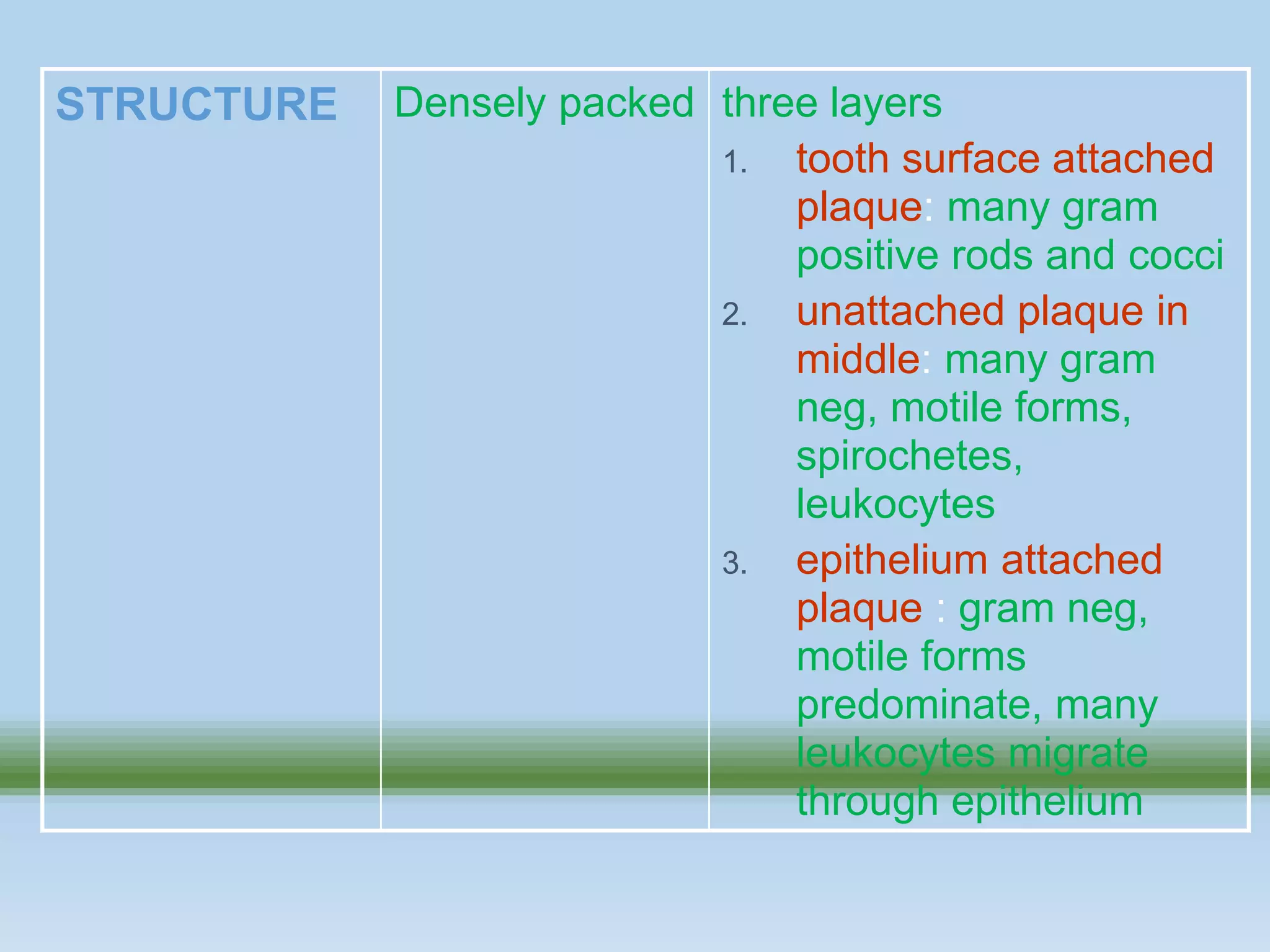


























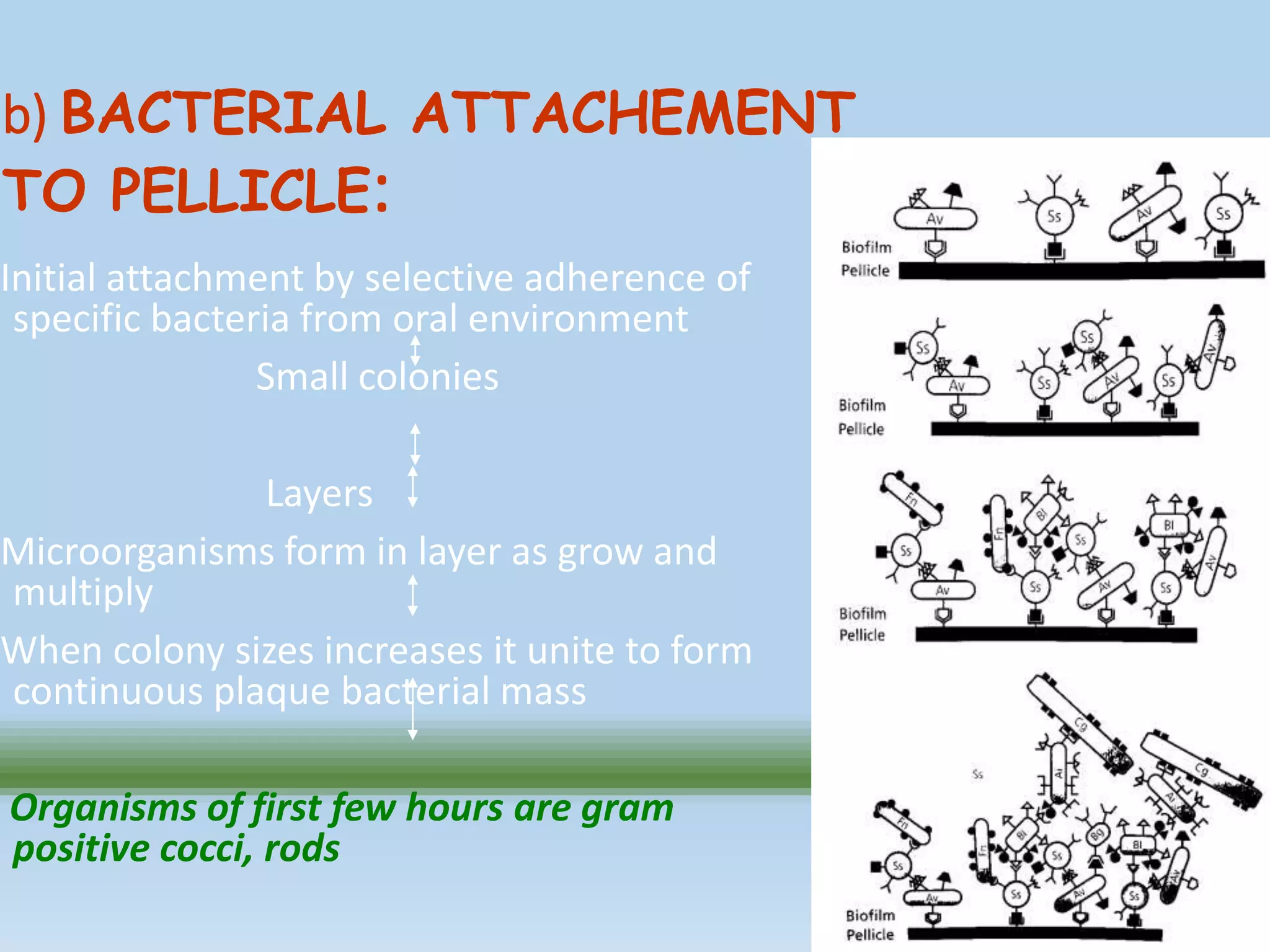

















































Dental plaque is a biofilm that forms on teeth. It is made up of bacteria, salivary components, and food debris embedded in an extracellular matrix. Plaque forms in stages - first, a protein pellicle forms on the tooth surface. Bacteria then attach to the pellicle and begin to colonize. As the bacteria multiply, they produce a matrix material between them made of carbohydrates, proteins, and lipids. Over time this leads to the development of a mature dental plaque biofilm.