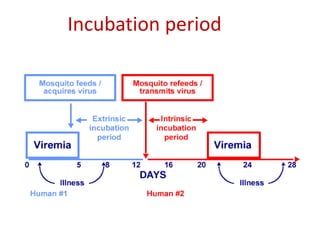
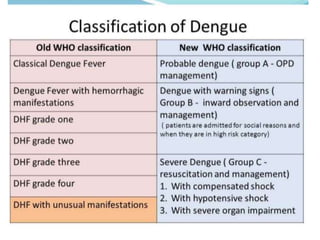
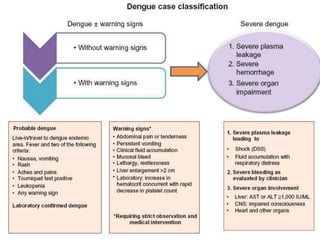
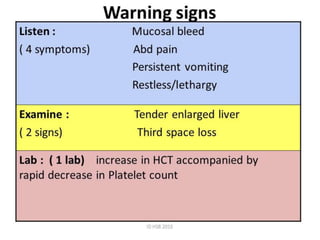
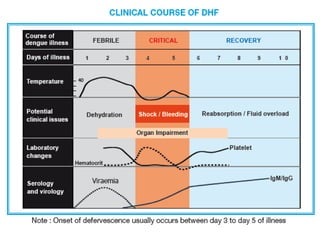
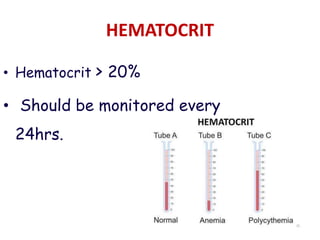
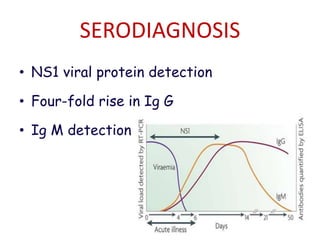
The document discusses Dengue virus infection, focusing on the role of the Aedes aegypti mosquito and the virus's biphasic fever illness caused by various dengue strains (DENV 1-4). It details the incubation period, pathogenesis, immune response, critical warning signs, and management protocols for patients, including assessment, treatment, and discharge criteria. The management varies by severity, categorized into outpatient, inpatient, and intensive care unit levels, emphasizing the importance of monitoring fluid balance and hematocrit levels.














































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)




![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)