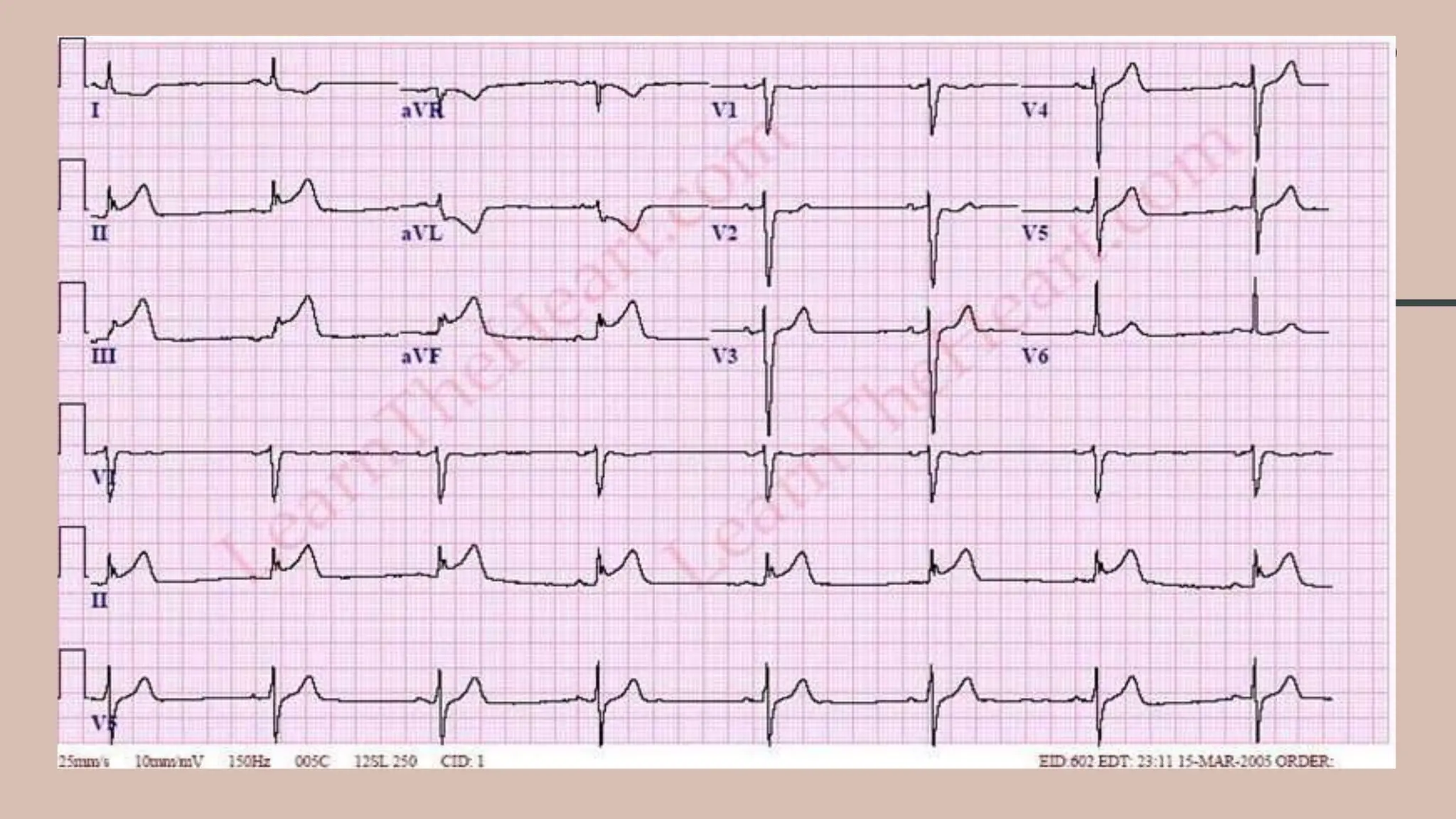
A 67-year-old male presented with sudden onset of chest pain for 20 minutes. Clinical examination found tachycardia and signs of heart failure. ECG showed ST elevation myocardial infarction (STEMI) involving the anterior wall. The patient was diagnosed with STEMI and underwent primary percutaneous coronary intervention (PCI). During the procedure, the culprit lesion was identified in the left anterior descending artery and treated with stent placement. Post-procedure, the patient was started on dual antiplatelet therapy and anticoagulation medication. He was monitored in the intensive care unit and later transferred to the cardiology ward for further management of risk factors and secondary prevention.








![ECG
CRITERIA
• ST-segment elevation (measured at the J-point) two contiguous
leads :
1. 2.5mm in men < 40 years
2. 2mm in men 40 years
3. 1.5mm in women in leads V2–V3
4. 1mm in the other leads [in the absence of left ventricular (LV)
hypertrophy or left bundle branch block LBBB)].
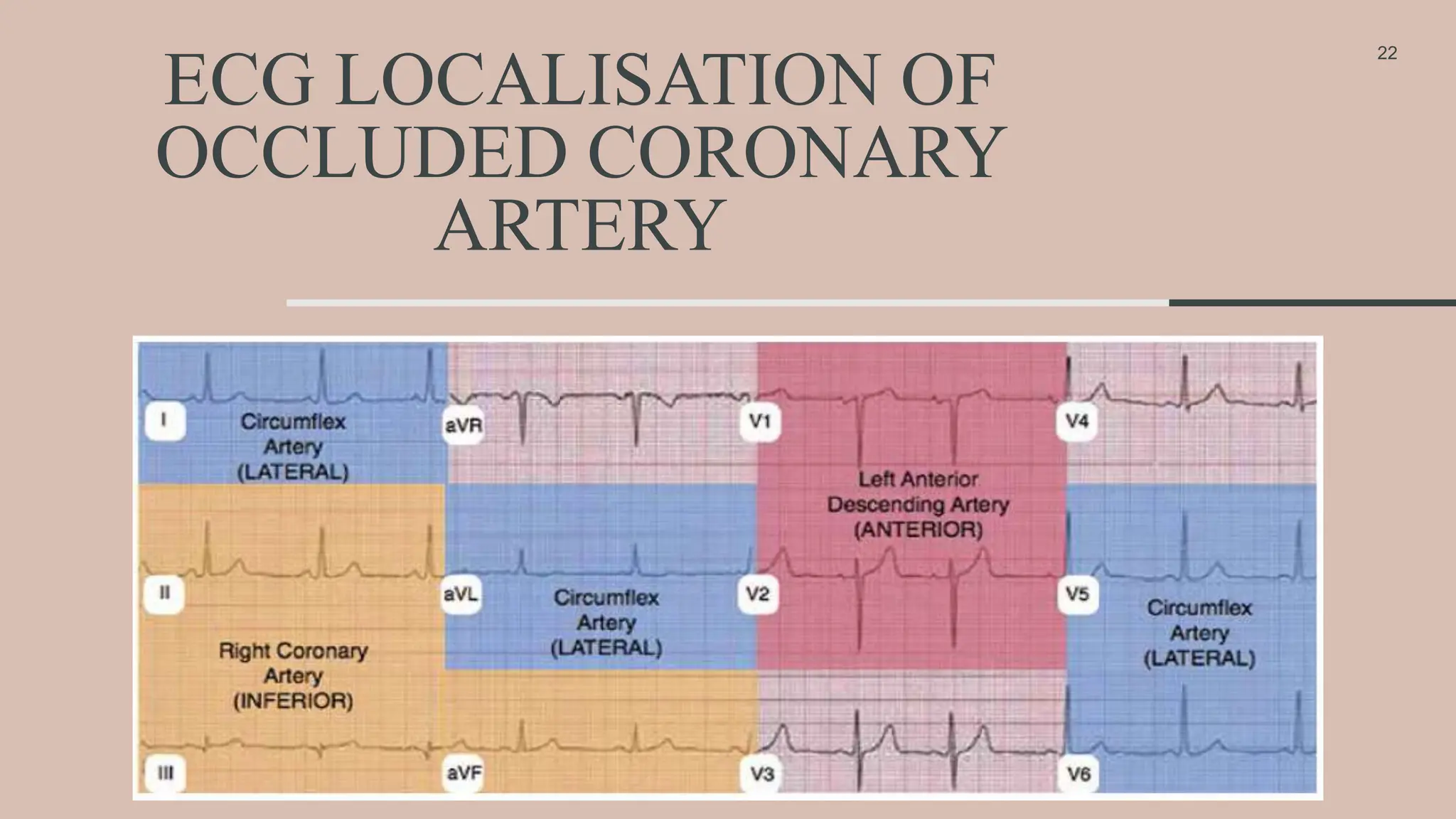
• Inferior wall MI :
1. Right precordial leads (V3R and V4R) for ST-segment elevation ( to
identify concomitant right ventricular (RV) infarction ).
• Posterior MI :
1. ST-segment depression in leads V1–V3
2. Concomitant ST-segment elevation 0.5mm in leads V7–V9
21](https://image.slidesharecdn.com/stemippt-231230070917-1549028d/75/STEMI-PPT-for-acute-coronary-syndome-acute-MI-21-2048.jpg)